In a recent article in Critical Ultrasound Journal from July 2013, the authors (Italians, of course! – they always do things ahead of everyone!) discuss the utility of contrast enhancement for solid organ evaluation in trauma patients. So, the FAST scan will assess for free fluid from injury, but we dont know what that injury is through a simple FASt scan. With contrast, we can better visualize the solid organs and assess for injury. The authors say it best, “Computed Tomography (CT) is the standard reference in the emergency for evaluating the patients with abdominal trauma. Ultrasonography (US) has a high sensitivity in detecting free fluid in the peritoneum, but it does not show as much sensitivity for traumatic parenchymal lesions. The use of Contrast-Enhanced Ultrasound (CEUS) improves the accuracy of the method in the diagnosis and assessment of the extent of parenchymal lesions. Although the CEUS is not feasible as a method of first level in the diagnosis and management of the polytrauma patient, it can be used in the follow-up of traumatic injuries of abdominal parenchymal organs (liver, spleen and kidneys), especially in young people or children.”
The thing to keep in mind is that this is actually not new – but evolving and getting spoken about more and more – as the authors state: “The first results in the literature indicates the use of CEUS in patients with blunt abdominal trauma after the FAST (Focused Assessment with Sonography in Trauma) or the US, in hemodynamically stable patients with a history of low-energy trauma [1,4,6]. CT is reserved in cases of severe trauma, with clinical suspicion of multiorgan lesions and cases with inconclusive CEUS [6].”
How does contrast work sonographically? Read on : “The contrast agents eco-amplifiers are able to modify the acoustic impedance of tissues, interacting with ultrasound beams and increasing the echogenicity of the blood. The contrast media (CM) ultrasound (USCA, UltraSound Contrast Agent) consist of microbubbles containing inert gases and surrounded by membrane stabilizers. The power of echogenic microbubbles and acoustic impedance depends on the size of the microbubbles. The microbubbles, unlike the tissues and the free gas, are not simply passive reflectors, but expand and compress in response to the stages of compression and rarefaction of the acoustic wave, with increasingly large hikes in diameter. The non-linear oscillation of microbubbles determines the emission of frequencies of said second harmonic with a frequency which is twice the insonation. Through the use of specific software, low acoustic pressures and an algorithm of specific processing, it is possible to selectively display the signals from the CM, separating the signal of the microbubbles from the one regarding the tissue. This particular signal is identified in real time by means of two main algorithms: Pulse Inversion (PI) and Contrast Pulse Sequence (CPS) [7,8]”
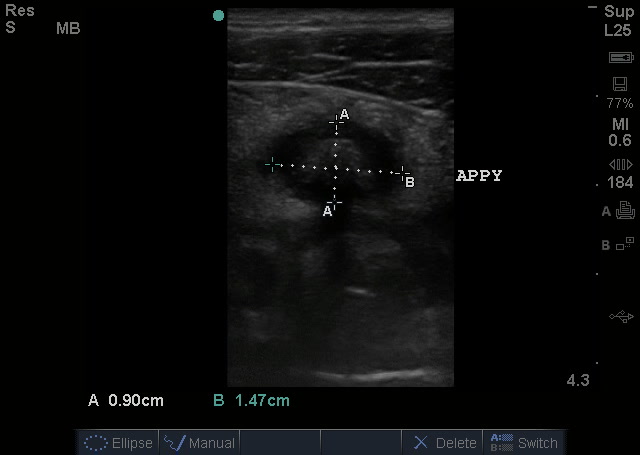
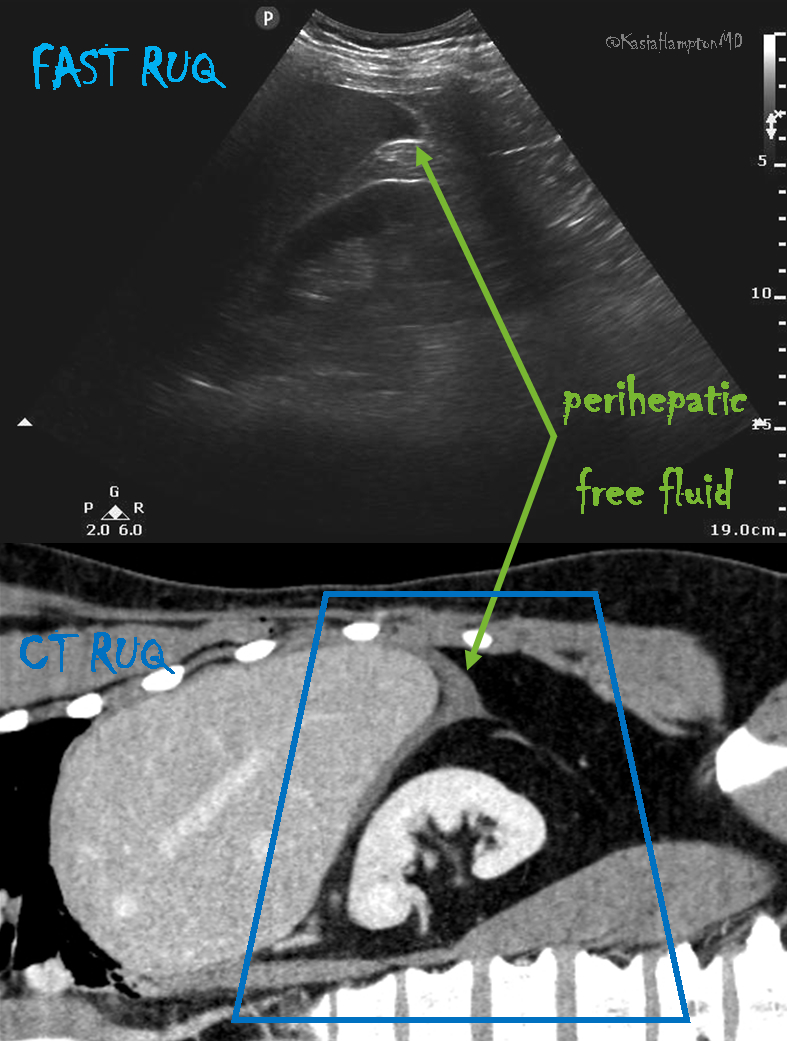
Here are some images from the authors in the article that makes the point:
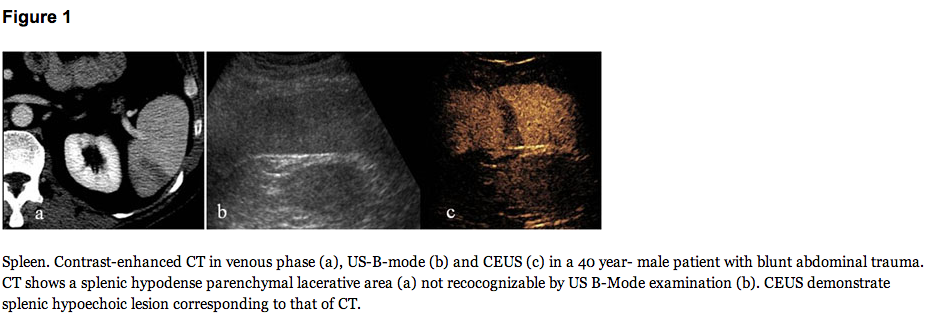
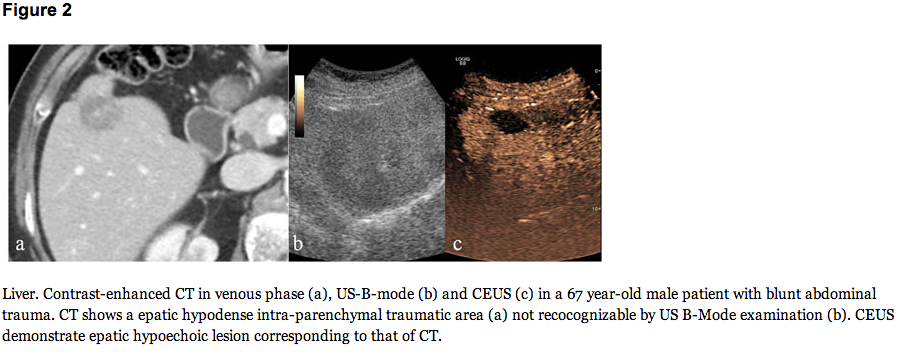
The conclusion? What to make of all of this?: “In the low-energy trauma and in hemodynamically stable patients, the US can be used as a first-level examination; when US detect intra-abdominal fluid CT examination is need. In the high-energy trauma the use of US as first line diagnostic is superfluous and damaging and the use of CT without and with i.v.c onstrast material is imperative. In order to reduce the radiation dose, particularly in young people or children, CEUS has an important role in the follow-up of conservatively treated traumatic injuries of the abdominal parenchymatous organs (liver, spleen and kidneys) diagnosed by CT [39,40]”
Read the article to get even more details on how the future of ultrasound will be, hopefully…here.