When I read this message, a light shined so bright inside my little head, that I had to share it. I got the usual emails from AIUM (American Institute of Ultrasound in Medicine), a multi-specialty organization with thousands of members, who educate/study/encourage/collaborate on issues related to ultrasound in medicine. But, the email that came out today, a message from the new AIUM President, discusses with such ease and obviousness about how ultrasound should be integrated into medical school education.
I have been to a few of the national AIUM conventions and my most recent post about it discusses one of the best days of my life, the course in NY at AIUM2013 about ultrasound integration to medical school curriculums where the experts spoke of their experiences, their advice, their ideas ….followed by a panel of medical students who shared their point of view of how it affected their education. It was amazing! Even now, when i think about it, i am inspired, and continue to be excited about how we are starting to do the same at Stanford School of Medicine. I have posted about the reactions that Ultrafest (a free medical student workshop in California) brought to everyone, including what UC Irvine’s Dean Clayman stated about it all. It was quite honest and encouraging. All of this, brings me to this message that i keep reading over and over again. Is it because 2013 is the Year of Ultrasound? Well, likely so, but for that reason and so many more, I just cant stop reading it – please read it below, especially the end when the link to the Ultrasound in Med Ed portal is introduced.
Dear Colleagues:
I believe there is no more important issue facing ultrasound than its incorporation into undergraduate medical schools’ curricula. Many of you saw the visionary presentation of Dean Richard Hoppmann, MD, at the 2012 AIUM Annual Convention in Phoenix, Arizona. Here at New York University School of Medicine, Uche Blackstock, MD, RDMS, an emergency department physician, is developing a multidisciplinary collaborative integrated preclerkship and clerkship curriculum. Consider the following:
It’s another typically busy day at the medical center. A critical care fellow supervises a senior resident placing ultrasound-guided central vascular access in a hypotensive septic elderly patient in the medical intensive care unit. In the outpatient surgery suite, an anesthesiologist prepares a patient for rotator cuff surgery by performing an ultrasound-guided interscalene brachial plexus block for regional anesthesia. In the echocardiography lab, a cardiologist assesses a patient admitted the night before with a non-ST segment elevation myocardial infarction for wall motion abnormalities and cardiac function. An obstetrics and gynecology attending performs a pelvic ultrasound examination on a young woman being ruled out for an ectopic pregnancy, appreciates an intrauterine pregnancy, and discharges the patient home safely.
Over the last 20 years, ultrasound performed at the bedside, by clinicians, has revolutionized the way medicine is practiced. In these diverse cases, the use of ultrasound was critical in providing patients with effective and quality clinical care. Although currently being used for diagnosis, management, and procedural guidance by physicians in numerous and diverse specialties, a significant gap currently exists between what medical students are being taught and how they are expected to practice on completion of their training. Future physicians will be expected to be familiar with the use of ultrasound in their clinical practice, regardless of specialty. At this time, medical educators have a unique and timely opportunity to use ultrasound at the bedside as an innovative teaching modality in the undergraduate medical curriculum.
Handheld ultrasound will transform how medical students are taught in the preclinical curriculum as well. Students will never experience learning medicine the same way. They will be able to scan a live model and appreciate the gallbladder as its lies within the main lobar fissure of the liver. They will have a deeper understanding of the cardiac cycle by viewing the diastolic and systolic phases of a live beating heart. During clerkships, students will learn how bedside ultrasound can be used to make important diagnoses and to allow them to safely perform critical procedures. Bedside ultrasound as a teaching tool will enhance what students have learned traditionally and help reinforce important concepts.
An integrated ultrasound curriculum will require a multidisciplinary collaborative effort by a medical school faculty. This approach will ensure that students receive comprehensive exposure to ultrasound from all perspectives. Medical educators are responsible for ensuring students are well equipped for future clinical practice. Ultrasound, as I see it, will have a dual role in undergraduate medical education. First, it can and should be incorporated into preclinical learning to teach anatomy, physiology, and pathology. Second, there is almost no clinical clerkship, as outlined by the scenarios above, that does not already or else will soon utilize bedside ultrasound. The future is now.
The AIUM’s Ultrasound in Medical Education Interest Group, chaired by David P. Bahner, MD, RDMS, has developed an outstanding online portal to assist those with an interest in integrating ultrasound into medical school curricula. This one-stop clearinghouse includes a mentor program; educational information from multiple organizations; and a tool kit that features curriculum examples, links to online lectures, sample proficiency assessments, tips on discussions with medical school leadership, instructor pools, equipment, and more. We encourage you to explore the Ultrasound in Medical Education Portal. If you know of additional resources that should be included, e-mail MedEd@aium.org.
In closing,
AIUM membership for students, residents, and fellows allows these individuals access to helpful ultrasound-related resources and the opportunity to network with experts in medical ultrasound–an excellent complement to the clinical training they receive. This membership category is $25 and offers students the full array of member benefits. The students of today are the future leaders of the AIUM. I hope you will share this opportunitywith those with whom you are in contact.
Sincerely,
Steven R. Goldstein, MD
AIUM President
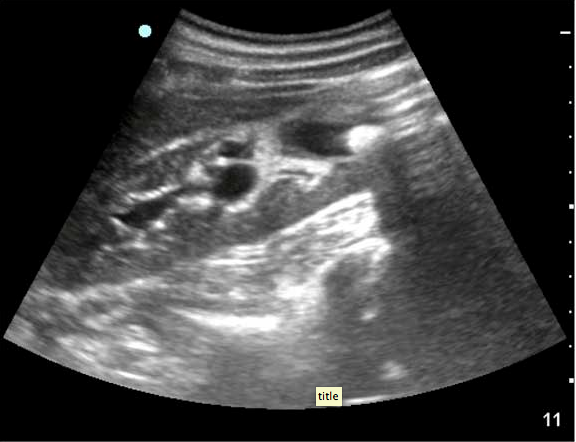
 1. Use your liver as an acoustic window.
1. Use your liver as an acoustic window.  Sound waves will travel through liver to the heart, allowing you to visualize the heart. Often one can even place the probe slightly to the right of the xiphoid process, to allow for better liver visualization, and then adjust your depth to be able to look past the liver to the heart. Without the liver in view, gas scatter will affect your image acquisition.
Sound waves will travel through liver to the heart, allowing you to visualize the heart. Often one can even place the probe slightly to the right of the xiphoid process, to allow for better liver visualization, and then adjust your depth to be able to look past the liver to the heart. Without the liver in view, gas scatter will affect your image acquisition.
 1. Start high and start medial – Place your phased array probe just next to the sternum, starting just under the clavicle. If you don’t see the heart there, slide down a rib space, and fan through that space to find the heart. Continue sliding down rib spaces, until you find it.
1. Start high and start medial – Place your phased array probe just next to the sternum, starting just under the clavicle. If you don’t see the heart there, slide down a rib space, and fan through that space to find the heart. Continue sliding down rib spaces, until you find it.

 Lastly, it can be very difficult in both subxiphoid and parasternal long views to differentiate epicardial fat pad from pericardial effusion. One tip: epicardial fat is seen anteriorly and has echogenicity within it, while pericardial effusion is seen posteriorly or inferiorly and is anechoic, but can travel anteriorly if large enough to become a circumferential pericardial fluid collection. Despite this tip, clinical correlation is needed.
Lastly, it can be very difficult in both subxiphoid and parasternal long views to differentiate epicardial fat pad from pericardial effusion. One tip: epicardial fat is seen anteriorly and has echogenicity within it, while pericardial effusion is seen posteriorly or inferiorly and is anechoic, but can travel anteriorly if large enough to become a circumferential pericardial fluid collection. Despite this tip, clinical correlation is needed.