US Director Emeritus, Stanford Emergency Medicine
Process Improvement Director, Stanford Emergency Medicine
Co-Chair, Case Review Committee, Stanford Emergency Medicine
In the march 2013 issue of Western Journal of Emergency Medicine, a study done that has been described as having generalizability, as the ultrasound scans were by many different levels of physicians, prospectively, during a trauma assessment for pneumothorax, has caused quite a bit of discussion. Mostly due to some of the limitations of the study. It is great that a prospective study with some generalizability is seen, but I wonder about the details in the methodology. They begin by discussing the importance and relevance of ultrasound for pneumothorax:
“Rapid diagnosis and treatment of traumatic pneumothorax (PTX) is important to prevent tension physiology and circulatory collapse in patients with blunt and penetrating trauma. Supine chest radiograph (CXR) is traditionally employed; however, it misses up to 50% of PTXs.1 Thoracic ultrasound (TUS) was first described in 1995 for diagnosing PTX in humans when Lichtenstein noted that the absence of comet-tail artifacts and lung sliding were associated with PTX.2 Since then ultrasound has become a validated method of examining the pleura in multiple settings. In 2011 the Eastern Association for the Surgery of Trauma gave a level 2 recommendation for the use of ultrasound to identify PTX in its practice management guidelines.3In most studies TUS has been found to have favorable results. In Lichtenstein’s study,2 TUS had a sensitivity and negative predictive value of 100% and 96.5%, respectively, for the detection of PTX in the intensive care unit setting.4 Dulchavsky5 subsequently demonstrated that this modality has a sensitivity of 95% in the detection of PTX in patients at a Level 1 trauma center. These reports used plain radiography as the gold standard: a diagnostic modality known to be inaccurate in the detection of PTX.6 In subsequent studies using dedicated chest computed tomography (CCT) as a reference standard, sensitivities of TUS have ranged widely from 49% – 98%, while finding that it is still consistently more accurate than supine CXR.7–13 Studies in which TUS is performed by emergency physicians (EP) for traumatic PTX have reported even higher sensitivities ranging from 86–97% with specificities of > 99%.14 While these latter numbers are desirable, they have the potential limitation of being less applicable due to a higher skill level of the sonologists involved. The actual performance of TUS for PTX would likely vary based on the sonologist’s skill and experience. The current investigation set out to determine the test characteristics of TUS for traumatic PTX in the hands of a large heterogenous group of potential sonologists representative of typical clinicians involved in trauma care.”
The full abstract is shown below:
“Introduction:
Prior studies have reported conflicting results regarding the utility of ultrasound in the diagnosis of traumatic pneumothorax (PTX) because they have used sonologists with extensive experience. This study evaluates the characteristics of ultrasound for PTX for a large cohort of trauma and emergency physicians.
Methods:
This was a prospective, observational study on a convenience sample of patients presenting to a trauma center who had a thoracic ultrasound (TUS) evaluation for PTX performed after the Focused Assessment with Sonography for Trauma exam. Sonologists recorded their findings prior to any other diagnostic studies. The results of TUS were compared to one or more of the following: chest computed tomography, escape of air on chest tube insertion, or supine chest radiography followed by clinical observation.
Results:
There were 549 patients enrolled. The median injury severity score of the patients was 5 (inter-quartile range [IQR] 1–14); 36 different sonologists performed TUS. Forty-seven of the 549 patients had traumatic PTX, for an incidence of 9%. TUS correctly identified 27/47 patients with PTX for a sensitivity of 57% (confidence interval [CI] 42–72%). There were 3 false positive cases of TUS for a specificity of 99% (CI 98%–100%). A “wet” chest radiograph reading done in the trauma bay showed a sensitivity of 40% (CI 23–59) and a specificity of 100% (99–100).
Conclusion:
In a large heterogenous group of clinicians who typically care for trauma patients, the sonographic evaluation for pneumothorax was as accurate as supine chest radiography. Thoracic ultrasound may be helpful in the initial evaluation of patients with truncal trauma.”
So what are the limitations? They describe a few of them:
The technique: “The TUS examination consisted of the consecutive sonographic interrogation of every intercostal space between the clavicle and the diaphragm on each hemithorax. Scans were performed in the mid-clavicular line. On the left side, if cardiac motion was encountered in the mid-clavicular line, the probe was moved laterally to the left anterior axillary line and the pleura seen in the remaining intercostal spaces was evaluated until the diaphragm/spleen was encountered. To use the ribs to assist in the identification of the rib spaces and the pleura, the probe was placed in a longitudinal plane for the entire exam.” So, would this have increased their sensitivity or specificity as they include all rib spaces? Not too sure. Is this truly generalizable if the technique is different than how most perform the quick E-FAST? no. The main reason for the technique, i imagine, is to find the lung point which is far more specific for pneumothorax.
The Probe and Machine – The low frequency curvilinear probe was used on an older ultrasound system – SonoSite Titan. Could this have affecte their results? Would the increased resolution of a linear probe have helped their evaluation on the newer machines? It is possible, but by how much? who knows.
The comparison group: “Not all subjects underwent CCT and instead just had CXR and clinical observation. It is possible that some patients in this latter group had radio-occult PTX that may have been visualized on CCT leading to misclassification bias. Such a bias could result in a lower sensitivity rate for both TUS and CXR, however would likely not affect the accuracy of these tests for determining clinically significant PTX.” It is tough to have a standard and if only the chest CT group were compared, it may have had different results.
Im hoping to see more studies like this one where more generalizability is seen, and not studies done only by the experts, so that we can have a true assessment. It is best done using the technique most commonly performed (using only the second intercostal space and mid clavicular line and trying to ind the lung point if absence of lung sliding is seen) at multiple-sites, with increased power to the study, all compared to a CT as the imaging gold standard. But, i can dream, as that is quite difficult to accomplish, and the authors did a pretty nice job with what they had, got pretty good numbers of subjects – something to ponder….
For a prior post on pneumothorax and a link to the CHEST meta-analysis, go here.
For a SonoTutorial post on pneumothorax ultrasound, go here.
Another study stating that ultrasound can be used to assess post=procedure pneumothorax published in June 2013 of JUM, go here.
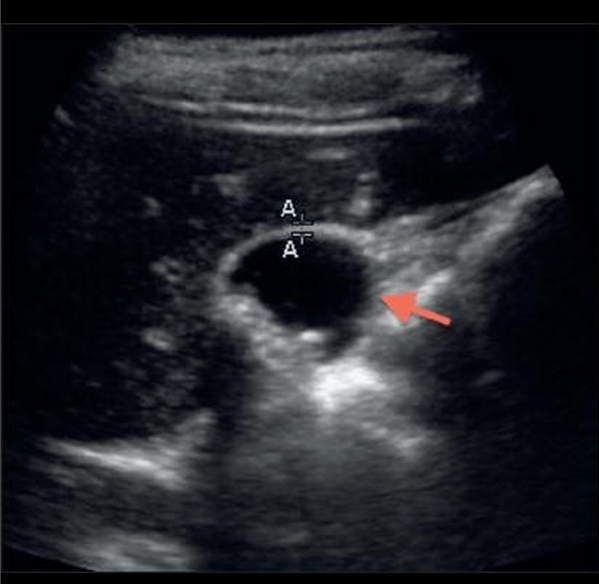
Western Journal of Emergency Medicine must be great proponents of bedside ultrasound! I love that journal! Of course, I am biased as I am one of the section editors, but these cases deserve mention. There have been quite a few in the March 2013 issue and this case in particular is a great review of renal ultrasound and what to lookout for in bedside ultrasound. Limited renal ultrasound typically involves an evaluation for hydronephrosis, but it is important to know what normal ultrasound anatomy looks like, as you may identify something else…. Dr. Marzec et al. at USC do a great job at discussing their case, describing their ultrasound, and giving a literature review on the finding. The case:
“A 45-year-old male with no previous medical history presented to the emergency department (ED) with 1 week of hematuria and left flank pain. The patient had noted that over the preceding 4 days his urine had progressed from a pink color to dark red. He had also experienced left flank pain that was sharp, non-radiating, and increasing in severity over the week prior to presentation. He denied a history of renal calculi, weight loss, fevers, fatigue, or abdominal masses. Upon physical examination, his vital signs included blood pressure of 157/89 mmHg, heart rate of 64 beats/min, temperature of 97.4 °F, respiratory rate of 18 breaths/min, and oxygen saturation of 99% on room air. The patient appeared comfortable. His abdomen was soft, non-tender and non-distended. The patient had left-sided costo-vertebral angle tenderness to palpation. There was frank hematuria in the urine sample at bedside. Subsequent microscopic analysis revealed > 50 red blood cells and 4–10 white blood cells. Bedside emergency ultrasound (EUS), initially performed to look for hydronephrosis, showed ….”
To read on the case, what happened, and a great review of the literature of ultrasound’s utility with this finding compared to other imaging modalities, go here.
The May 2013 issue of EM News highlights one of the basic, yet most difficult, ultrasound applications to perform. It is one of the most common abdominal applications given how common the disease process shows itself in the emergency department. Nice work to Dr. Hisset, a first year resident! from Louisiana, on writing this review.
The case: “A 54-year-old woman presents to the emergency department with four days of fever, abdominal pain, nausea, and vomiting. She reports that all of this started after eating pork at a casino buffet. She is not jaundiced on exam, but has severe pain to palpation of the entire abdomen, worst in the right upper quadrant with a positive Murphy’s sign. Her blood pressure is 96/52 mm Hg, pulse is 110 bpm, and her temperature is 100.4°F. Fluid resuscitation is started, and a bedside ultrasound is performed.”
To find out what they found and a description of the application in a concise format, go here.
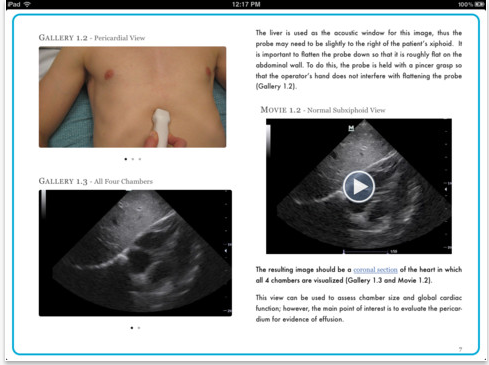
LLLLLLLLet’s get ready to UltraSoooooooouuuuuuuuund!!!! It’s what we have all been waiting for! It’s finally here! Weighing at a meager zero pounds (since it’s on the iPAD, oh yeah!), another amazing product of Drs. Mike Mallin and Matt Dawson of ultrasoundpodcast fame, and authors including experts in bedside ultrasound from around the world (and little ole’ me too). I’d like to present the SECOND volume of the Introduction of Bedside Ultrasound ! And, as Mike and Matt say it best, “If you already own Volume 1….” (which include topics in basic ultrasound applications & more filled with visual image and video clip tutorials – unlike any other “text”book that you have ever owned!) “…..this is much better. If you don’t yet own Volume 1….they’re equal…..get them both.” – Yes, trust me, you will not be disappointed. You can also get Volume 1 on inkling chapter by chapter purchasing ability where you can read it on your iPHONE too!)Take your iPAD to the bedside, place it on the ultrasound machine, or both to help guide your ultrasound education and that of others! Volume One pics:
Volume Two involves topics on TEE (which is an up and coming application of bedside ultrasound in cardiac arrest), MSK, Right Heart, EMS, Medical Education, Gallbladder, more Nerve Blocks (that’s where I come in..heehee :), PIV, Soft Tissue, DVT, Appy, Peds, Diastology, and much more! 364 pages of interactive content, with HOURS of video demonstrations and tutorials. – doesn’t that make you drool!?! In volume two picture: …do you know what technique that is? you will…
To hear them speak on it, and to get a taste of perfection, go here.
March 2013 was a great month for ultrasound case reports and publications – especially in Western Journal of Emergency Medicine! Once again, the team from USC highlight a case where ultrasound is used at its best. As they state: “its greatest asset lies in the ability to rapidly make the diagnosis of a time-sensitive medical condition, enabling the [emergency phsyician] to mobilize resources and expedite treatment, which might otherwise be delayed. The use of [emergency] US for the evaluation of scrotal injury from blunt trauma exemplifies this point.” Isn’t it great when you include ultrasound in your examination of a patient who you will call a specialist for anyway, but to also describe the injury to them in detail, including whether there is hematoma, blood flow, or other findings – and expedite specialty care? YES! They do an excellent job in describing scrotal anatomy, the risks of missing injuries, and the findings of the case while reviewing scrotal ultrasound and the literature around it as well. This is worth the time to read it!
The case: “22-year-old male with no significant past medical history presented to the Emergency department approximately 3 hours after he was in an altercation, during which he sustained multiple blows to the head, stomach, and genital area with a large flashlight. His primary complaint was of severe testicular pain.
Physical examination revealed a calm, well-developed male in mild distress due to pain. Vital signs included a blood pressure 132/85 mmHg, heart rate of 90 beats per minute, respiratory rate 16 breaths per minute, and temperature 98.9°F. On examination of the genitals, the penis was normal. His scrotum was enlarged to approximately the size of a grapefruit, and the overlying skin was erythematous. The scrotal area was exquisitely tender to palpation, making it impossible to reliably identify or examine either testis, despite the use of parenteral opioid analgesia. A urinalysis was obtained, which was normal and notably negative for blood.” The ultrasound study showed:
Read on more, as there are more videos, and a great description of scrotal trauma and injuries with an evidence based review.
A great pictorial review of testicular ultrasound and pathology, go here.
This case is one where if I were the doctor, my immediate response may have been hidden from the patient. Inside voice would NOT have stayed in. Wow! Dr. Torregrossa and the team at USC discuss a case published in March 2013 Western Journal of Emergency Medicine of a patient where there obviously was no bedside ultrasound performed for the duration of his symptoms. “How long was that?” you may ask… ONE YEAR! Wow! He saw his doctor (check), he got a chest Xray (check), he got an EKG (check). Good thing he finally got an ultrasound study ….
The case: “61-year-old male with a 1-year history of bilateral lower extremity swelling and a chronic cough was referred to the emergency department (ED) for an abnormal echocardiogram. The patient also reported experiencing intermittent episodes of chest pressure. He stated that he was referred from his doctor after he received a cardiac echocardiography examination that showed possible mitral valve vegetations. On review of systems, he also admitted to intermittent chest palpitations. On physical examination, his vital signs included a blood pressure of 127/75 mmHg, heart rate of 80 per minute and regular, respiratory rate of 18 per minute, pulse oximetry of 98% and temperature of 98.0°F. The rest of the physical examination was normal. An electrocardiogram demonstrated normal sinus rhythm and the chest radiograph was unremarkable. ED bedside ultrasound (EUS) showed….”
To read on the topic so that you will know some of the literature behind it – go here.
In the March 2013 issue of Western Journal of Emergency Medicine, Dr. McKaigney highlights a case that illustrates there is more to a thoracic and right upper quadrant bedside ultrasound study than just free fluid, renal and gallbladder evaluation. You must look everywhere and appreciate when something looks abnormal. I always say, know what NORMAL looks like, because when you see something abnormal, you’ll identify at least that, then want to find out what that abnormality is by further testing.
The case: “A 35-year old male presents to the emergency department (ED) with what he describes as right-sided upper back and flank pain, which he attributes to a “cupping” procedure the day prior. The cupping procedure is an alternative medicine practice that uses local suction to theoretically stimulate blood flow and promote healing. He had no previous issues with the procedure. On further history he reported having had approximately 6 weeks of intermittent fevers, cough, anorexia and general malaise. He had seen multiple naturopathic physicians for these complaints, before an urgent care visit one week earlier. At that time, he had been started on azithromycin and doxycycline for a presumptive diagnosis of pneumonia. In the interim week he reported an improvement in his febrile symptoms and overall well-being. He was an otherwise healthy heterosexual male, without drug use or travel outside the country. He had no known sick contacts.
On physical examination his vital signs included a blood pressure of 116/75 mmHg, a heart rate of 119 beats per minute, and a respiratory rate of 20 breaths per minute. His temperature in the ED was 36.2°C. Oxygen (O2) saturation was 97% on room air. The patient was alert, and appropriate with no signs of respiratory distress. Pertinent physical findings revealed typical, non-tender cupping marks on his back. More concerning was an absence of breath sounds on the right side of the chest on auscultation. His abdomen was soft and non-tender. The remainder of the physical examination was non-contributory.
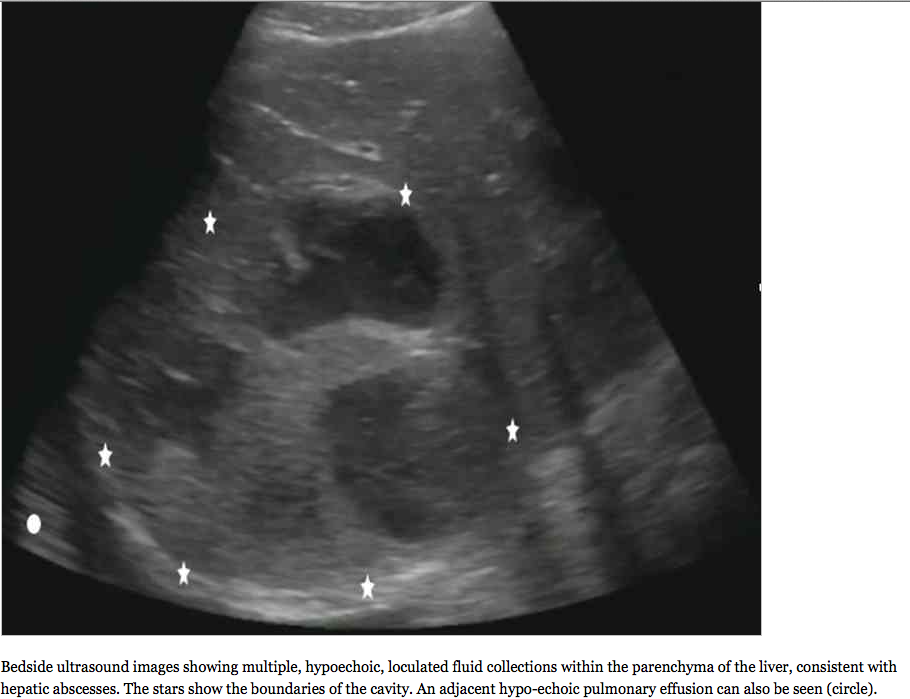
The initial diagnostic test ordered was a chest radiograph, which showed 80% opacification of the right hemithorax, consistent with pneumonia and associated parapneumonic effusion seen in Figure 1. A bedside ultrasound was subsequently performed in the ED, initially in order to examine the size of the pleural effusion in which a startling discovery was made…..”
So, “what is that?” – you may be asking…. and what happened to the patient, what can be done about it, and what is the evidence based review on the topic? Read on as Dr. McKaigney does an excellent job in discussing it all….here
Once again another great case by Drs. Teresa Wu and Brady Pregerson in EP Monthly. Whenever I read their cases, I can actually imagine myself going through the case too. This is especially true for this one, as it is a prime example of how ultrasound can get you the diagnosis immediately, and how ultrasound can be utilized in the elderly and demented nursing home patients who get sent to the emergency department for “she just doesn’t seem normal” or, in this case, “abdominal distension”. Trust me, both can actually end up with the same diagnosis. It’s also a great entry as it speaks of a procedure that all emergency physicians should know how to do – it is too easy!
The case: “72-year-old male brought in by his nursing home aide for abdominal distension. He has a history of dementia and is primarily bedridden at baseline. The patient cannot give any reliable history, but on physical exam, his otherwise thin abdomen shows obvious signs of suprapubic distension. Your intern recaps his vital signs, which include tachycardia at 120 bpm, a blood pressure of 190/86 mmHg, a respiratory rate of 20/min, and a normal temperature and O2 saturation.”…. So, the differential diagnosis? Well, you should always think of the most emergent first, like an abdominal aortic aneurysm, which can also be diagnosed by ultrasound immediately – as discussed in a prior post of another elderly patient with altered mental status. (To see more sonocase posts in evaluating the altered patient, go here). Other badness? perforated bowel, volvulus, mesenteric ischemia, hemorrhage…. Oh, the list keeps going on and on when you have an elderly patient, a demented patient, a nursing home patient – or, in this case, it was all of the above!
Whenever I am evaluating the elderly patient with abdominal complaints, I think bedside ultrasound immediately (of course, with a very low threshold for CT scan since they can have anything happen! – and let’s be honest, they aren’t the ones we think about when we talk of the radiation risks… But, healthcare bill/cost? That’s a whole other conversation…). After as best of a history and physical exam that I can get (it can be challenging when they are demented and no caregiver at the bedside! Calling the nursing home is always done but usually they are too sick or the person on the other end of the line gives limited information), I bring my ultrasound machine and explore their abdomen: FAST (which also gives you a good look at the kidneys for hydronephrosis), Aorta, Gallbladder, Bladder, Bowel, +/- Pelvic/Testicular (depending on exam). Doing that may give you the answer, as in the case highlighted above…. to find out what they found and what happened to that patient, read on here. Trust me, you’ll love it.
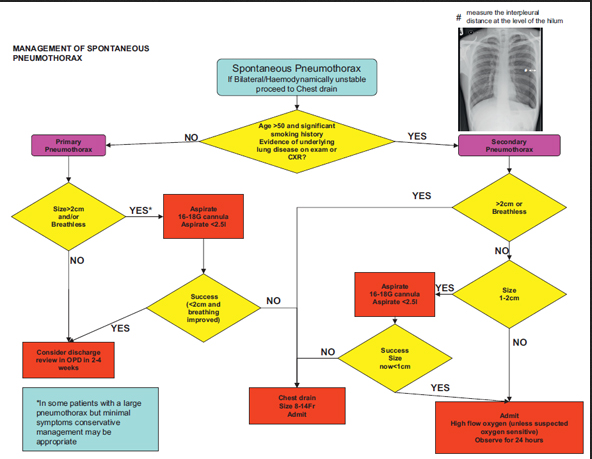
If there ever was a post worth reading about pneumothorax, this excellent review by EM Lyceum was too good not to pass along to everyone. Now I don’t know about you, but I always get asked the questions about chest Xray versus Ultrasound, what to do when only the ultrasound shows the pneumothorax (because you know it’s better than Chest Xray! as discussed in a prior post), when to order that CT chest, and how should you treat it: nothing? pigtail? small chest tube? large chest tube? EM Lyceum does a great job in reviewing this using literature to back it up. There have been more studies that haven’t been mentioned with regard to ultrasound and pneumothorax diagnosis, and the sensitivity and specificity of chest xray is stated pretty high as prior studies tend to do (with more accurate and recent ones stated by EM Lyceum to be lower (in the real world that we work in). And, there was a great meta-analysis in Chest Journal speaking of which imaging modality was better, chest Xray or ultrasound. Go to the EM Lyceum site and read-on to grasp the answers to all the questions! Thank you EM Lyceum – this was awesome!
The American Institute of Ultrasound in Medicine (AIUM) 2013 conference in New York City was the best AIUM I have ever been to, and it continues to open up my mind (having my ideas run wild!) to so many things that ultrasound will do for medicine, while reminding me of the up-to-date studies that clarify many ultrasound-related topics in medicine. It is true that Ultrasound should be considered first with many conditions, and as an emergency physician, point-of-care bedside ultrasound is definitely an example of that. It absolutely should also be implemented into medical school education to have a head-start at becoming an excellent physician. AIUM has an emergency and critical care section too and I have taken full advantage of the information there, as should you. (Jason Nomura has gathered all AIUM13 tweets for your reading pleasure for all AIUM13 topics)
YOU = Year of Ultrasound!
This post is a one part of a 4-Part Series where I discuss all the lectures, panel discussions, and events that i attended there, and what every emergency doctor should get out of it, and the literature that backs it up or discusses the controversy – all through my and other’s twitter feed with the addition of some links to relevant material.
The first day was one of my favorites! It was the Ultrasound in Medical Education panel discussion from the experts, coordinated by Dr David Bahner, who has recently published study after study after study after study with regard to how he incorporated ultrasound into medical education and how to standardize ultrasound education. You can even listen to and view the whole course if you have an AIUM membership, by going here. Dr. Richard Hoppman, the Dean of University of South Carolina, who has also published study after study after study after study on this topic, also gave his pearls and wisdom from the Dean’s perspective. (Hear/View his interview with UltrasoundPodcast by going here.) Other experts also gave their expertise in this hot topic, as they have also published and highlighted study after study after study after study as shown below in the tweet and panels’ pearls from the course (as well @SonoMedED tweets who provided more highlights for the course): Ultrasound in Medical Education (I posted on the comparison of Ultrasound to physical exam previously – but there is so much I need to add to it now!)
a. Provide clinicians with resources to guide medical student training in clinical ultrasound to better provide care for their patients
b. Provide educators with the resources and tools to coordinate clinical ultrasound in medical curricula
c. Provide researchers with evidence based resources to create and validate new knowledge through innovative and rigorous academic pursuits
d. Provide administrators with data and contact personnel at respective medical institutions who are applying novel ultrasound education across the medical spectra
e. Provide medical students with a one-stop portal to navigate current United States medical student ultrasound education and opportunities to get in school
1. David Bahner – This would involve changing curricula, training faculty, acquiring equipment, support staffing, quality assurance, OSCE or SDOT, establish “best-practices.” In 2004, the medical organizations differentiated & defined ultrasound into four categories: Comprehensive, Focused, Procedural, Physical exam aid
2. D. Lichtenstein – “They call me Dr. Lung, but I do more.” There are exciting ways to show medical students the importance of ultrasound….New territories of ultrasound: mesenteric ischemia (“a bowel that doesn’t move is a dead bowel”), pneumoperitoneum, increased ocular use. Took 15 publications in order to publish the BLUE protocol that reviews 10 signs of lung US. Respiratory failure: BLUE http://crashingpatient.com/wp-content/uploads/2011/07/Lichtenstein-Slides.pdf … ; Circulatory failure: FALLS (if no B lines then good systolic fxn; if B lines then bad systolic function); Cardiac Arrest: SESAME protocol (lung sliding (if pneumothorax- immed interv), echo, then IVC and AAA at your discretion: http://www.slideshare.net/nswhems/the-arrested-patient … Lung Ultrasound in Critically Ill for Limiting Radiographs (LUCIFLR) project – to decrease CT and chest Xrays (but not to eradicate Xrays “or LUCIFLR will = LUCIFER”). Lung ultrasound can limit the need for chest X-rays in the ICU and the ED.
3. Creagh Boulger – speaking on literature review of ultrasound curriculum for medical students. MT “@SonoMedED: Medical students effectively use ultrasound in just 5 min in some situations.” [Even beating clinicians in diagnosis! See: this study.] . Study after study has shown that medical students benefit from ultrasound in medical education. How to fit it into the schedule? what they did – online didactics (like Fox’s iTunes series), then 16 weeks of hands-on, concluded with a checklist based assessment. Why teach it? Increases Anatomy Learning, increases diagnostic ability in radiology, assists in spatial relationships, and they see “live anatomy” with better ability to learn physiology in real-time.
5. John Pellerito – how to incorporate US into med school: buy in from Dean, faculty training, facility space, US equipment, MULTI-specialty involvement (emergency medicine, radiology, critical care, obstetrics, medicine, surgery). US in med school: online didactics, most time must be spent with hands-on: knobology, anatomy, physiology, pathology (- partner with pathology /radiology dept to show how ultrasound correlates with histology/specimens and CT/MRI [they will learn to read those better too by learning ultrasound!]). Society of US in Med Ed (SUSME) website to see sample curriculum. The Challenges of incorporating US into Medical Education: maintenance of longitudinal curriculum, keep faculty enthusiastic, budget for new equipment, space needs. MT“@SonoMedED: Challenges with med stud ultrasound educ 4yr curriculum, keep faculty interested. pic.twitter.com/UnRSCGs0vk”. Who to Train them? First will be faculty, then the seniors can teach the juniors. Essentials im developing an US curriculum: didactics and hands-on training, integration into anatomy, physiology, physical exam and diagnosis skills, clinical clerkships, and requires student assessment and image archiving and review. Faculty/Facility needs: classroom, bedside, anatomy lab, stretchers, gel, towels, monitors, models (students or patients), faculty from multiple specialties
6. Amponsah/Jackson – from Wayne State : how they incorporate US in med stud curriculum: didactics, 2nd yr competency test, multi-specialty involvement. Where US helps med stud in anatomy learning: spatial relations, pathology, live anatomy pic.twitter.com/MCI972lryO . Need high faculty:student ratio. LCME requirements are key to getting ultrasound into medical school:
LCME requirements are a great way to advocate for ultrasound education as part of active learning for medical students …..The following LCME requirements can be satisfied with ultrasound: ED-5-A: A medical education program must include instructional opportunities for active learning and independent study to foster the skills necessary for life-long learning; ED-12: The curriculum of a medical education program should include laboratory or other practical opportunities for the direct application for the scientific method, accurate observation of biomedical phenomena, and critical analysis of data; ED-28:A medical education program must include ongoing assessment of medical student’s problem solving, clinical reasoning, decision making, and communication skills.
7. J. Christian Fox – From UC Irvine. pic.twitter.com/znUAea1wew . Bridging the gap between pre-clinical and clinical students with simulations: How to do it: transitioning from pre-clinical to clinical medical students: podcast, then hands-on with healthy volunteer, then task trainer, then recognize pathology on simulator, then standardized patient with pathology, then clinical rotation utilization by way of an OSCE pic.twitter.com/ix4Rl2X4WS “Sono-genic” models great to use- models with great US anatomy. Issues in real patients: obesity, COPD, pain- all limit scan ability but great for later training. Great models: Sono-Studs… Or, not so good: Sono-Mess MT“@SonoMedED: Terms for good sonographic models…Sonogenic…Sonolicious.” (Ah, I digress…). Solve issue of assessing pathology: simulation! Various simulators are on the market: http://Sonosim.com , http://bluephantom.com ,http://Vimedix.com , http://www.medaphor.com/ , http://www.medsim.com/ultrasim.html . MT “@SonoMedED: Dr. Fox signs up pts for modeling with various pathologies. Model pts with pathology compensated $80 for 4 hour session. Often challenging to schedule patients though.” Great way to get models who have pathology! Studies show increasing ultrasound performed in ED when increased medical student ultrasound learning, also that liver span size better when use ultrasound. Medical students are better with ultrasound in diagnosing cardiac disease when compared to cardiologists’ physical exam.
8. Michael Blaivas– The role of specialty organizations- AIUM, SUSME, WINFOCUS, and specialty specific: ACEP, SAEM, ACS, ACOG, ACCP, SCCM, Card, Rads. http://SUSME.org primary purpose is integrating US into med educ. http://WINFOCUS.org primary purpose to help proliferation of Ultrasound education, is worldwide, has detailed US educ curriculum, policy making depending on region/country. Summary- issues and specialty organization – how they help pic.twitter.com/ZsO9BKWa6B
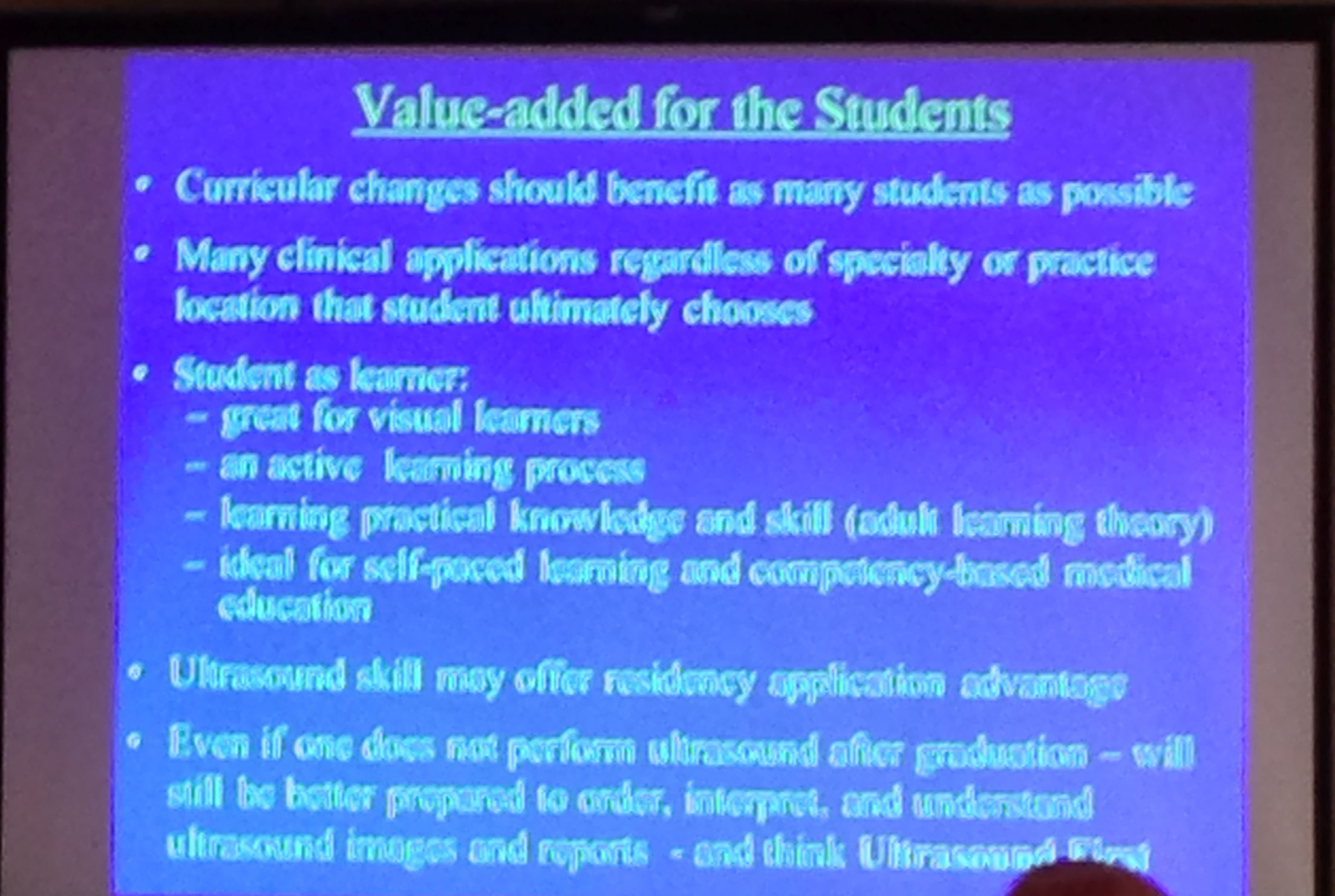
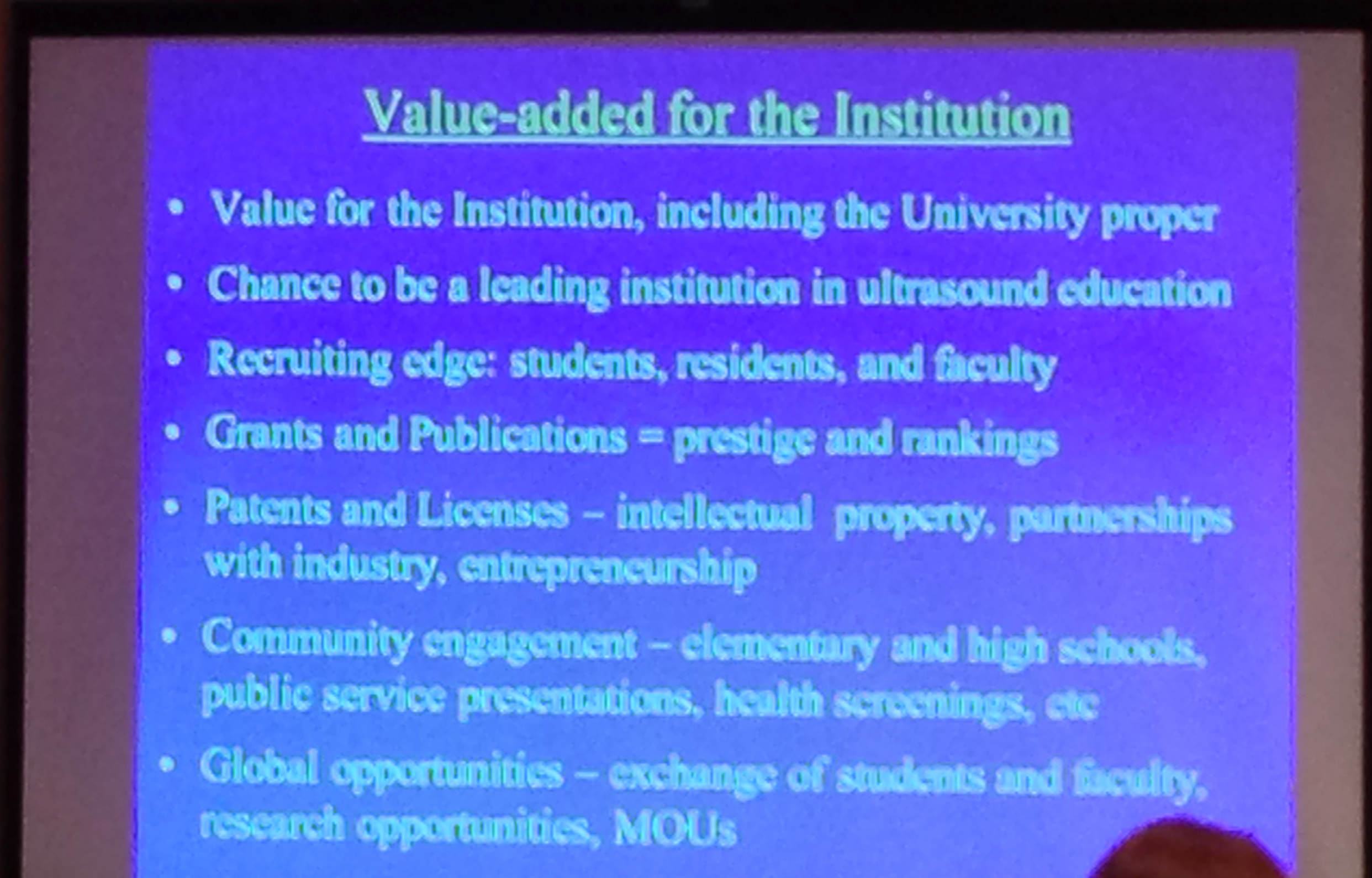
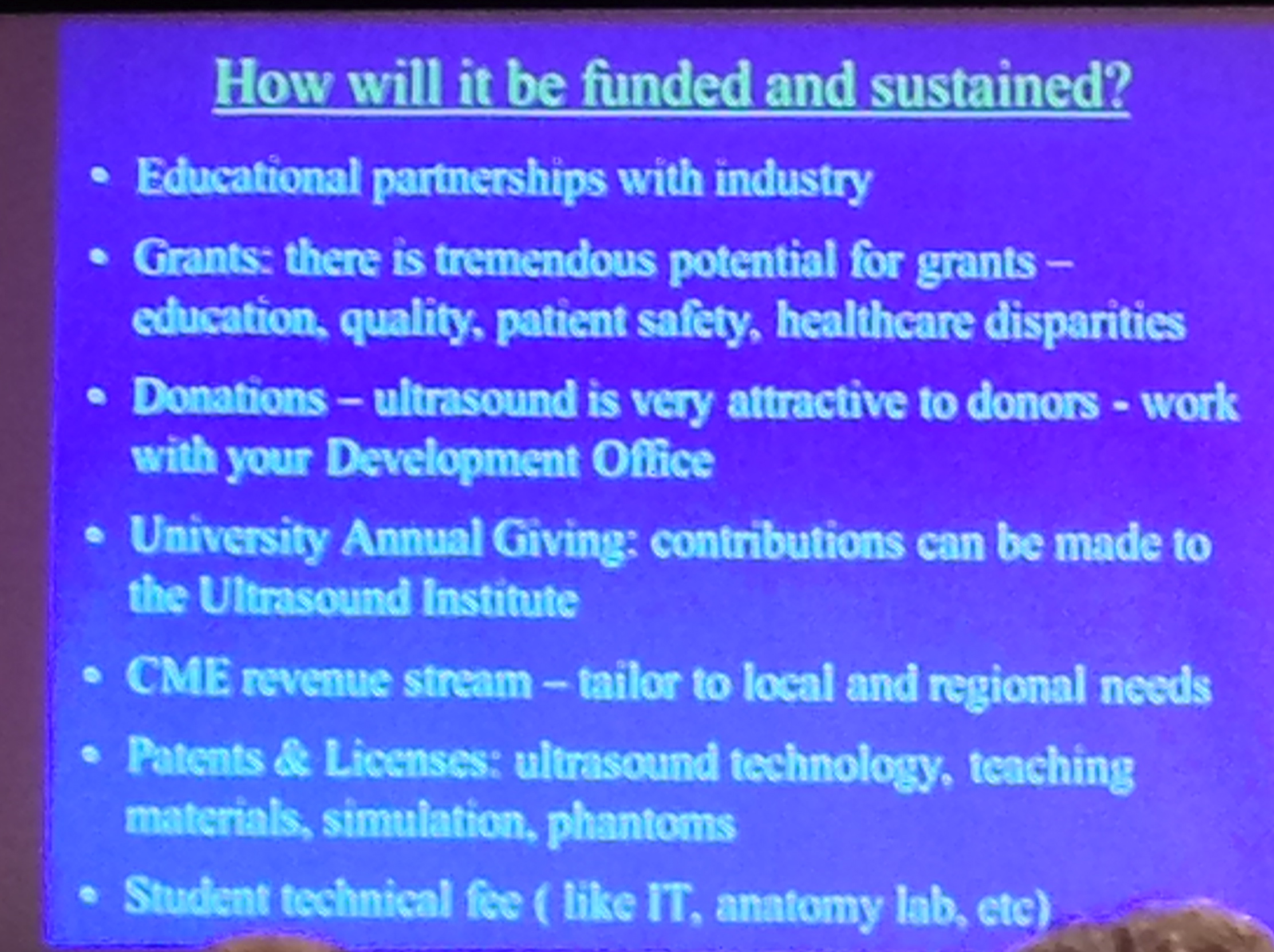
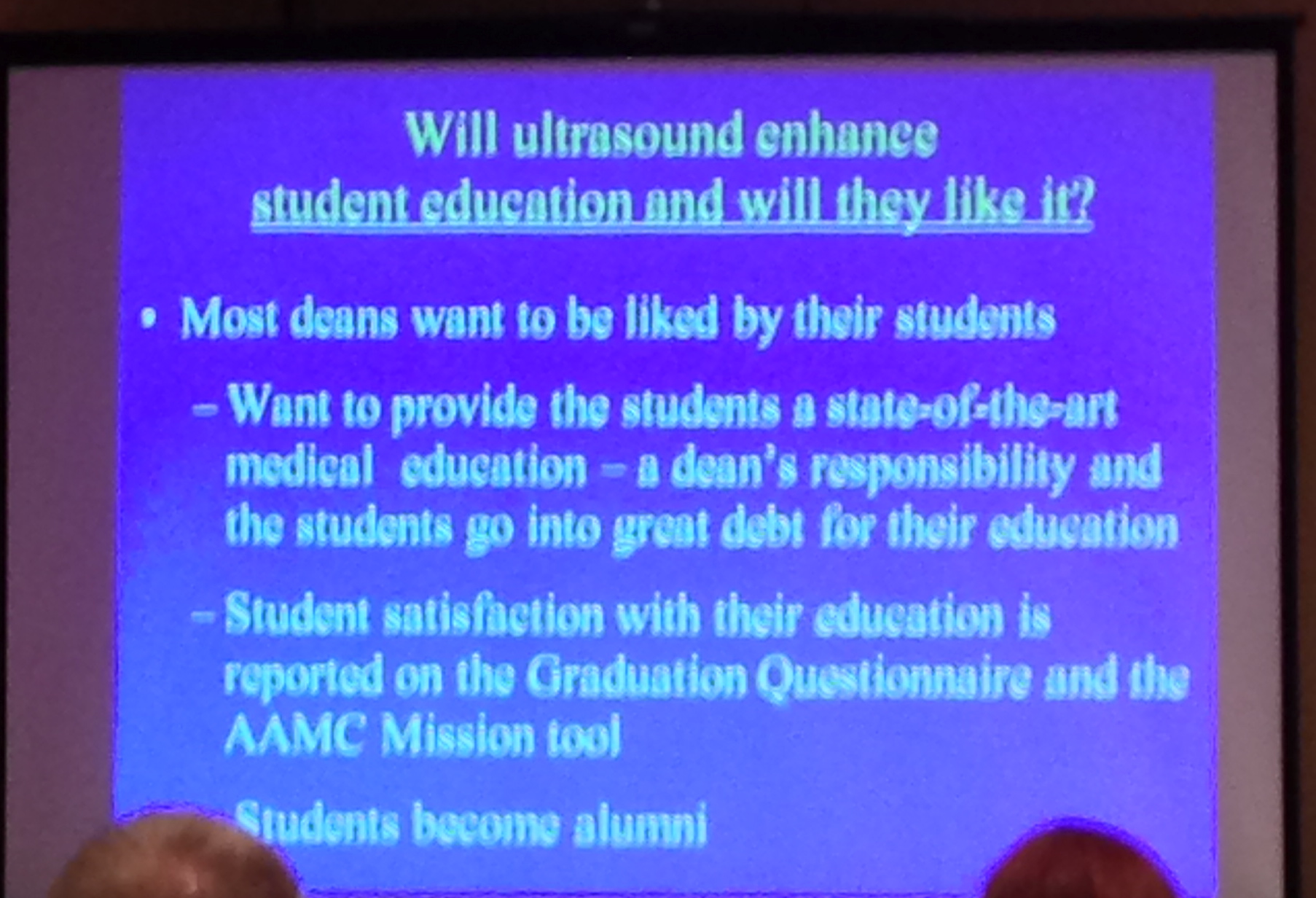
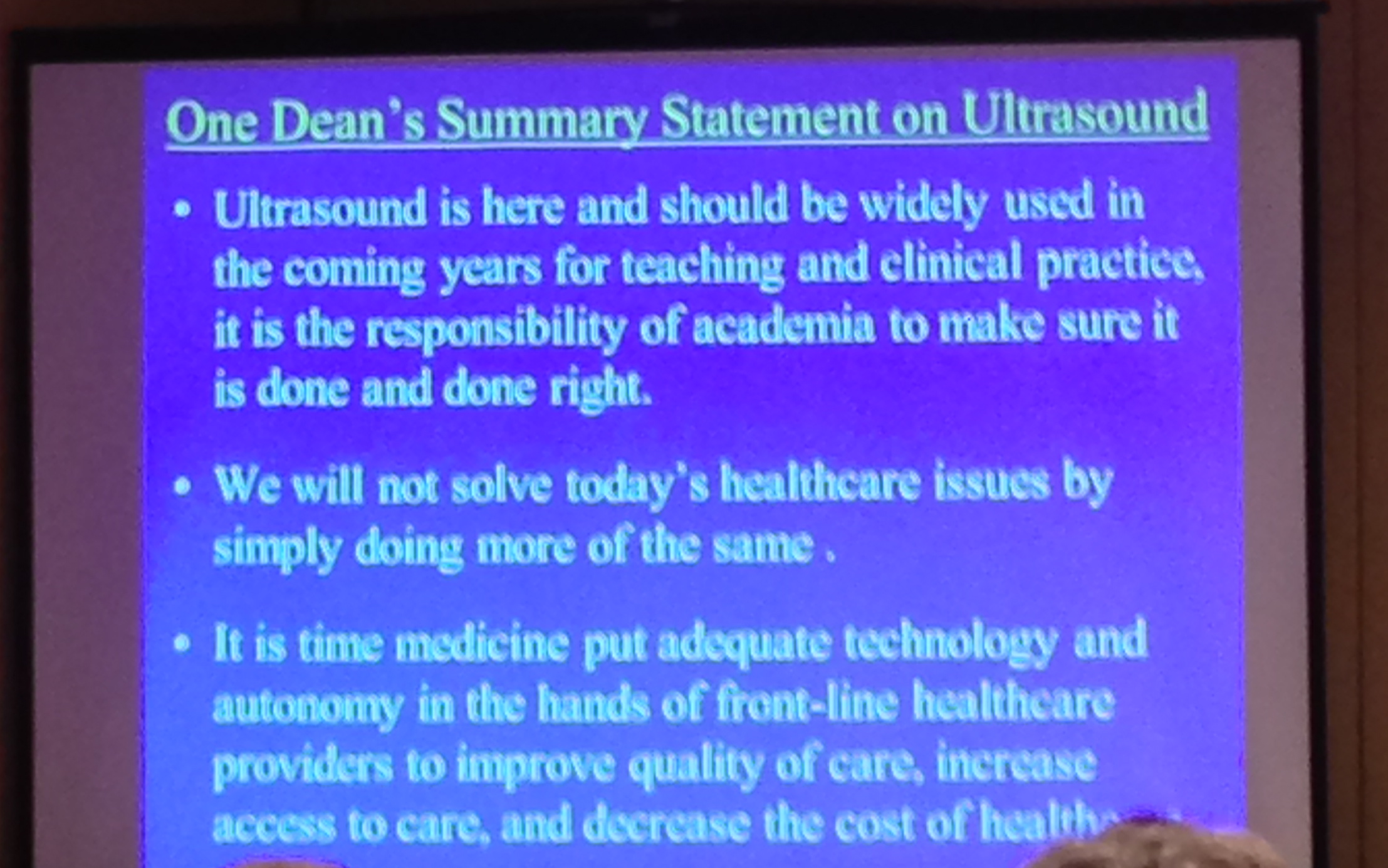
9. Dean Richard Hoppman – from University of South Carolina: pic.twitter.com/hAx4Iqv9rR . US in medical education- A Dean’s Perspective, how to get them on your side: how to get US in medical education- get medical students on your side, show US enhances medical education, satisfies LCME requirements, fits all types curriculum. When ultrasound becomes part of Step 2 exams is when you know we’ve arrived… [Wow! Can u imagine?!]….Ultrasound competency could be an advantage to residency application. Even if they don’t use US in residency, can order/ interpret/understand ultrasound and other radiology studies better, they’ll think Ultrasound First! How ultrasound adds value to institution pic.twitter.com/dzJt0VAaNE . Hopefully one day ultrasound training will be a requirement for medical school graduation. How to fund ultrasound for your institution pic.twitter.com/uItTHJj2Jb . MT“@SonoMedED: Universities increasing focus on entrepreneurship. patent ultrasound ideas or devices. Help fund program” Great idea by Hoppmann -> MT “@SonoMedED: Advocate option for donors to contribute to medical school ultrasound programs.”The new stethoscope? MT“@SonoMedED: Grants supply equipment for med studs, even handheld units. pic.twitter.com/5t9wbOtsef” medical students love it, medical students become alumni, alumni become donors. Great way to advocate for it pic.twitter.com/TnxBLjhsJn. Dean’s summary message to all: Get it. Learn it. Do it. Teach it. For your patients & healthcare pic.twitter.com/LfUQv2SbJK . Yes!!-> “@SonoMedED: Great insight from Dean Hoppmann. pic.twitter.com/VcW1BUmbRl”
10. Teresa Liu – from GW (the one who is putting it all together for med studs at AIUM/SAEM/ACEP). White paper on ultrasound in medical student education is in progress. ACGME now incorporates ultrasound into EMed and RRC doing same for rheumatology. Medical students can get involved in specialty organizations/journals focused in ultrasound: JUM, Acad Med, SUSME/SAEM/AIUM/ACEP. Lower cost-Increased use! -> MT“@SonoMedED: Liu- need for making US tech more affordable to better penetrate into all specialties.”
11. Alex Levitov– curriculum and competency assessments: challenges & opportunities. Driving force for ultrasound are many clinical cases where it’s relevant & when time matters: its a busy day or patient critical.When people ask why – tell them this: pic.twitter.com/CUth7L3Vxj . US allows immediate diagnosis, immeidate data in patient care, & allow reassessment after intervention (CVC placement, chest tube, foley…). Competency in US- image acquistion in years 1/2 ; Simulators, clinical cases & they decide what to do next for years 3/4. US in meded-cardiac physiology usually rated low by medical students, but rated high after ultrasound used to enhance education. Best way to incorporate US in medical education- staged approach -& use clinical cases early, ask about interventions in clinical years
12. Vicki Noble– from Mass General – discusses Ultrasound Competency –NEJM article -Point of Care Ultrasonography shows how many use it . “Numbers” for image acquisition competency- should it exist? Arguments for & against exist. Outcome need to be different? “Consensus is great, paralysis is bad”-concept of plateau-do more of same if literature show numbers don’t matter may mean we should change. US competency numbers may be different for different ultrasound applications; numbers may not matter for some applications- testing image interpretation requires clinical integration & “next step” questions. Online ACEP US test: http://www.emsono.com/acep/exam.html
13. James Palma– from Georgetown – web based & organizational considerations in ultrasound in med ed – organ based approach – online didactics; hands on. web based US curriculum pic.twitter.com/l9fuWycluk
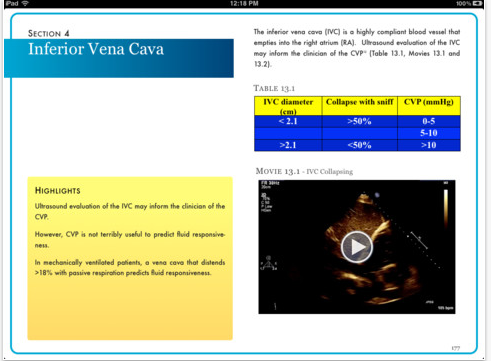
14. Last but not least – MEDICAL STUDENT PANEL !! Medical students panel discussing how #ultrasound helps them -going into different specialties pic.twitter.com/4B8IjKjtTQ . Ultrasound helps spatial relations in anatomy, great for MSK in real time (ie. rotator cuff movement), heart great to match with physiology (“it’s hard to understand heart physiology by reading a book, and so much better when you see the valves opening and closing and how the heart pumps”) . Great to see kidney ultrasound because anatomy dissection takes all abdominal organs out & can’t appreciate spatial relations. “@SonoMedED: Med Student Panel-Ultrasound physiology best demonstrated for IVC collapsibility and ejection fraction.” When asking medical student their preference: separate course versus full integration in different classes with regard to ultrasound into medical education: all wanted the latter – unanimously! . Story by a medical student: Psychiatric ward patient w/ abdominal pain got hand-held ultrasound by medical student showing cholecystitis- comprehensive ultrasound confirmed; OR that day. MT“@SonoMedED: Med Stud Panel-key to making integration of ultrasound successful: make it clinically relevant in 1st/2nd year.” “Ultrasound makes me feel that I can contribute to the team.”
15. Prior advances in Ultrasound in Medical Education has been highlighted by others: I have posted about how ACEP, AAMC, and AIUM last year has started speaking about ultrasound in medical education; UltrasoundPodcast have a great podcast about it and how to incorporate it here and here; WesternSono posted about this from the Canadian perspective with an amazing and fun talk pitching ultrasound training in medical education here; the world is advancing this goal as well!
Some of the great slides that grabbed my attention from the AIUM13 course: (apologies for the blurry iPhone images)
The Medical Student Panel:
The Course’s Faculty: aka – the All-Stars!
And, to conclude with great insight and words of wisdom for why ultrasound should be in medical education:
And what he has done to spread the gospel of ‘sound! – go here to read more and hear a speech done by the Dean of UC Irvine Medical School on why its so important to incorporate ultrasound into medical education for our patients.


 and
and