
Once again, our Stanford Ultrasound Workshop was a huge success. Why? Our instructors were phenomenal and from different specialties! Our participants were faculty from emergency medicine, internal medicine, critical care, surgery, and pediatrics! The ultrasound tips and tricks just kept on coming from our lecturers – and, everyone laughed at our jokes, which always makes things great. As always, I like to provide those tips and tricks to all of you (and maybe even some of the jokes), so that you can feel like you were there too!

Dr. Sarah Williams – First, the coordinator for the Stanford CME workshop welcomes everyone with a Star Wars phrase “Learning you are….May the force be with you, young padawans!” – always goes to a great start. She is also the creator of the Stanford Ultrasound Program and current Associate Residency Director (and the person who was kind enough to put up with my quirks and jokes to hire me as a fellow years ago). Her pearls on the EFAST: detects >600 cc (intraperitoneal) fluid, look around inferior pole in RUQ and subdiaphragm area of LUQ (free fluid develops first there!), it’s not good for pelvic fx/injuries (pelvic bleeding into pelvic cavity, and retroperitoneal, bowel gas obstructs view, bladder may be empty limiting visualization), it’s not done fast- FAST is part of RUSH, but dont rush the FAST. Look for your kidney, then look above it, around it and below it (thoracic fluid, morison’s pouch, paracolic gutter). FAST LUQ: higher, spleen smaller, stomach big -place knuckles on gurney, oblique probe in plane to ribs, free fluid can be between diaphragm & spleen. #ultrasound detects 15-20cc fluid in thoracic cavity, better than chest Xray. Have patient take deep breath to lower diaphragm. The longer the patient is supine (or trendelenberg) the better, so if you have a walk-in trauma, perform serial FAST scan. SX view: the liver is the heart’s protector, be sure to see it in view- it allows you to see the 4chambers. gas is heart’s enemy – if gas gets in the way, you cannot see the liver: slide probe laterally to patient’s right, get that liver in your view. For pneumothorax eval – use linear probe, find your ribs, ID pleur liine, decr gain (brightness) to see sliding better. Start high in midclav line, indicator to head – – then travel thru mult rib spaces to estimate size.

Dr. Laleh Gharahbaghian (since i cannot speak about myself, I let someone else write this part and promised I wouldn’t change anything – let us pray…): “With her usual stylish self, walking all around the workshop, giving hi-fives to everyone in her path, her dance moves came in handy as she spoke (can you point her out in this video from the mid 1990s of her past job?) – She is the current Director of the Stanford Ultrasound Program and Fellowship her pearls can be found below: Her pearls of Aorta US: use large footprint probe, if get gas, press down, takes time – as if you were reducing a hernia; start in the subxiphoid region, travel down thru to iliacs. Most AAA are infrarenal and may seem normal in size at sx and get large once you travel down. Doesnt evaluate for rupture – most AAA leak/rupture retroperitoneal – not detected by US (your FAST is neg) – correlate clinically to your patient symptoms and vital signs. Her pearls on Renal US: main indication: hydronpehrosis, but pay attention to everything (outside to inside); eval both kidneys AND bladder- without bladder, you wont know if the bilateral hydro may just be that they have to pee. If empty bladder, and bilateral hydro, then possible mass (if not chronic). If patient is >50yo with flank pain, dont forget to eval the aorta as well. Start outside to inside for pathology – free fluid around kidney, cyst from kidney, mass on kidney, stone within kidney, hydronephrosis. Her pearls on Gallbladder US: start in the subxiphoid region, indicator to patient’s right, use liver as window, fan thru it medial to lateral to find GB. Then, fan/eval in transverse & longitudinal planes. Fanning thru the GB is key- there’ll be sections where it looks normal, then you fan & a stone comes into view! See if the stone is mobile by turning patient and re-scanning to see if moved. Think of the number 4 (or multiples of it) with measurements: width 4cm, length 8-10cm, anterior GB wall <4mm, CBD 4mm at 40yrs old (adding 1mm for every decade beyond).

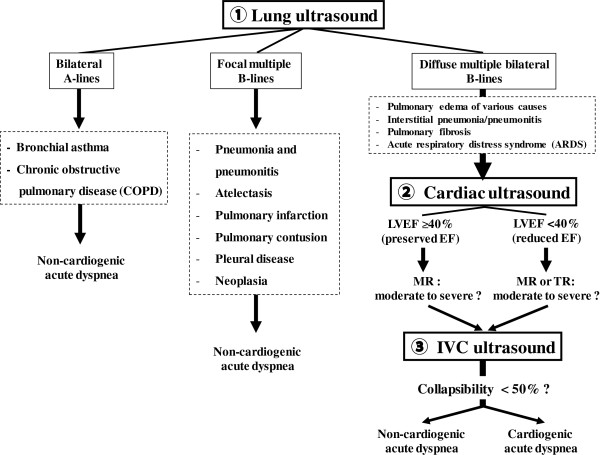
Dr. Phil Perera – our newest addition to the Stanford US team serving as the Director of US Research and the Associate Program Director gave quite an engaging talk on Echo and the RUSH protocol, putting it to action! As is highlighted by his Soundbytes website that is a free source of lectures for your viewing pleasure, he would keep asking the audience whether they would involve their consultants, if they would “write home to mom about this?!” The funny part is that one of the audience members responded with “I wouldn’t have to, she would call me before I get a chance.” Another participant concluded the point by saying, “You must work in a profitable community hospital.” Ah – gotta love the sarcasm! Phil continued his talk discussing when you should act fast by going through RUSH cases, giving props to others who also study and educate on resuscitation ultrasound. His pearls on Echo: PSL view is the favorite – lets you evaluate right ventricle size, left ventricle size and contractility, pericardial effusion, pleural effusion and mitral valve regurge; Echo should be done with IVC when thinking about fluid resuscitation – if hyperdynamic -can tolerate fluid; if hypocontractile, not so much; Echo can eval aorta too! PSL view visualizes ascending aorta and descending aorta; AP4 view shows descending aorta – look for aneurysm/flap. Intraperitoneal fluid and pleural effusion can be mistaken for pericardial effusion – know where your pericardium is! Pleual effusion in PSL view travels behind descending aorta; pericardial effusion travels in front of descending aorta. AP4 great for comparing RV and LV chamber size, contractility of RV and LV. To get the P4 view, slide lateral after parasternal views until get to apex, angle to body center. His pearls on RUSH: Case that inspired him: 67yo acute SOB, in shock h/o COPD/CHF/HTN, CXR neg, ultrasound showing the cause to not be sepsis, but cardiogenic shock. RUSH provides the answer to : sepsis? cardiogenic? hypovolemic? hypervolemic? tamponade? PE? trauma? tension ptx? AAA? First & most important is the cardiac echo: the PUMP, that’s why it’s first – lots of info from a single cardiac view (PSL). For semi-quantitative contractility eval: fractional shortening & EPSS are measured – PSL must be at approp long section. tamponade on #ultrasound – RV collapse during when it should fill (diastole)-also can see RA scalloping -do pericardiocentesis. pericardiocentesis: US studies show having pt in left lateral decubitus position & an apical view better for removing pericardial effusion than traditional SX technique. IVC – can use M mode to measure in both transv and long view 2cm from RA – can use your internal jugular as an alternate. Lung ultrasound – B Lines – think of fluids and your resuscitation when evaluating etiology of shock: FALLS protocol by Lichtenstein. Although rare, if your EKG has STEMI, do an ECHO – make sure its not a dissection before you start heparin!
 and
and 
Dr. Zoe Howard (our Director of Medical Student and Resident US Education) and Dr. John Kugler (coordinator for the internal medicine US elective and global health US instructor) spoke about the many awesome ways ultrasound can help with procedural guidance. The dynamic duo had awesome videos to assist in their lecture and went through the many procedures that can be done with US guidance. Their pearls on Procedural US: On central line access – first look for the vein before you prep the area; it’s possible that the vein you want (or the location of the vein you want) is not the best vein for the procedure. Your indicator should be to your left, the screen dot should be on your left, that way left means LEFT when you’re guiding your needle tip to the vein. On lumbar puncture – do it when you can’t feel the landmarks, when you only have one attempt, when you’ve already had one unsuccessful attempt. Use the ALiEM trick with a paperclip for drawing the straight line. On thoracentesis and paracentesis – make sure you view the area where there is at least 2cm of fluid between the probe and the lung/bowel to avoid lung/bowel puncture – it may not always be where you think. On pericardiocentesis – look for where the fluid is most, patient to left lateral decubitus position, and you’ll find that SX is not the best anymore. On nerve blocks – learn it, do it, and teach it! Your patients deserve it! Use the in-plane approach to visualize your entire needle, and use the dental syringe holder to have control over your syringe.







We then had 8 different hands-on stations with 11 different instructors (and 4 chickens used for central lines deserving of props, and lots of other simulators as you will see in the below pics)! Including those described above, we also had the above instructors (from left to right, top to bottom (hyperlinks take you to “other” images that come up when you google search their names)- Dr. Viveta Lobo – our current US fellow and future Director of the Visiting Scholars Program, Dr. Brita Zaia – our past US fellow and current Kaiser San Francisco Ultasound Director, Dr. Darrel Sutijono – US fellowship trained faculty at Kaiser Santa Clara and new to twitter and #FOAMed and the FOAM movement, Dr. Manish Asarvala – US fellowship trained at UCSF and faculty at Kaiser Santa Clara. Dr. Yoshi Mitarai – an emergency medicine/critical care specialist who recently saved a life while at the gym doing Zumba (yup, you read that right), Dr. Suzanne Lippert – a specialist in nerve blocks and international/global health who is faculty at Stanford EM. Dr. Jennifer Newberry – an MD JD (so, super smart) and one of our senior EM residents who is staying on as a fellow in healthcare/ public policy.











{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}