In a recent study in Pediatric Emergency Care, the folks at newark Beth Israel in New Jersey studied whether performing a pelvic ultrasound decreases length of stay. Now, we all can appreciate this – you have a pregnant patient with first trimester vaginal bleeding or abdominal pain, you see an intrauterine pregnancy without any risks/signs of heterotopic (which is incredibly rare anyway) – you’re done! You dont even have to wait for the beta hCG! Of course that decreases length of stay! Now, this wasnt the first study of it’s kind. Another study by Blaivas et al. basically did the same thing… 13 years ago! And by Burgher…. 16 years ago. And by Shih…. 16 years ago! There was a great review of pelvic ultrasound done in 2009 that shows its accuracy and utility too.
Well, here is what they state: abstract below
“OBJECTIVES: Diagnostic ultrasounds by emergency medicine (EM) and pediatric emergency medicine (PEM) physicians have increased because of ultrasonography training during residency and fellowship. The availability of ultrasound in radiology departments is limited or difficult to obtain especially during nighttime hours. Studies have shown that EM physicians can accurately perform goal-directed ultrasound after appropriate training. The goal of this study was to compare the length of stay for patients receiving an ultrasound to confirm intrauterine pregnancies. The hypothesis of this study is that a bedside ultrasound by a trained EM/PEM physician can reduce length of stay in the emergency department (ED) by 1 hour.
METHODS: This was a case cohort retrospective review for patients aged 13 to 21 years who received pelvic ultrasounds in the ED during 2007. Each patient was placed into 1 of 2 groups. Group 1 received bedside ultrasounds done by institutionally credentialed EM/PEM attending physicians. Group 2 received radiology department ultrasound only. Each group had subanalysis done including chief complaint, time of presentation, time to completion of ultrasound, length of stay, diagnosis, and disposition. Daytime was defined as presentation between 7 AM and 9 PM when radiology ultrasound technologists were routinely available.
RESULTS: We studied 330 patients, with 244 patients (74%) in the bedside ultrasound group. The demographics of both groups showed no difference in age, presenting complaints, discharge diagnoses, and ultimate disposition. Group 1 had a significant reduction (P < 0.001) in time to complete the ultrasound compared with group 2 (mean, 82 minutes [range, 1-901 minutes] vs 149 minutes [range, 7-506 minutes]) and length of stay (142 [16-2268] vs 230 [16-844]). Of those presenting during the day (66%), group 1 showed a significant reduction in length of stay (P < 0.001) compared with group 2 (220 [21-951] vs 357 [156-844]). Of those who presented at night (34%), group 1 showed a significant reduction in length of stay (P < 0.002) compared with group 2 (270 [16-2268] vs 326 [127-691]).
CONCLUSIONS: The use of ED bedside ultrasound by trained EM/PEM physicians produced a significant reduction in length of stay in the ED, regardless of radiology ultrasound technologist availability.”
Some interesting cases for your review:
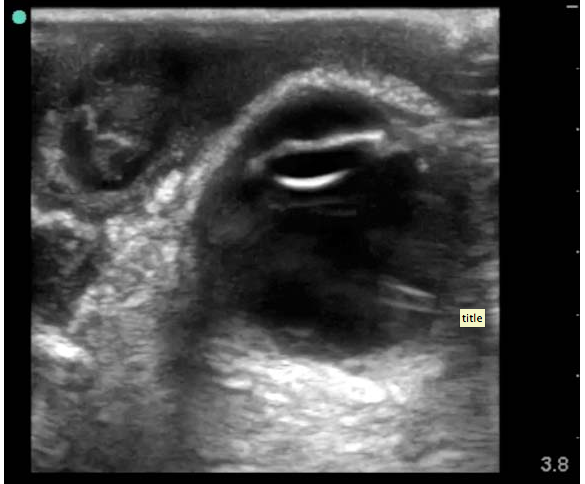
SonoCase: 30 yr old with pelvic pain, LMP 5 weeks ago, stable vitals, mild tenderness in suprapubic area, pelvic exam normal. Your Transabdominal pelvic view on ultrasound shows the below. What do you do next?
Well, we see a full bladder – which is a must if you actually care about your pelvic views – and we see a gestational sac with a double decidua sign – the earliest sign of an intrauterine pregnancy, BUT it is not enough to diagnosis a definitive intrauterine pregnancy – you need a yolk sac within your gestational sac to say that! So, get your endocavitary ultrasound probe and take a look (after emptying the bladder), you may just see the yolk sac!
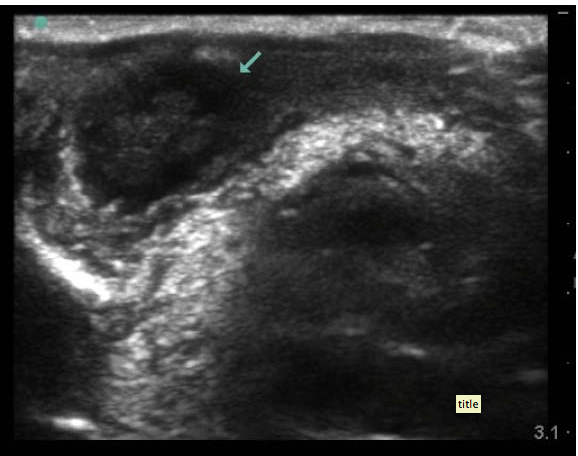
SonoCase: 24 yr old with pelvic pain, LMP 6 weeks ago, stable vitals, mild tenderness in suprapubic area, pelvic exam normal. Your Transabdominal pelvic view on ultrasound shows below. What is the diagnosis? What do you do next?
Well, there is an empty bladder (unfortunately), so the visualization is not its best, but while we slowly fan through the pelvis there is a fluid filled circular cystic-like structure with mild acoustic enhancement (brightness deep to it) which allows you to also see a gestational sac within the uterus. There is an ovarian cyst. Is that what’s causing the pelvic pain? Are you sure it’s not an ectopic? Not yet – get your endocavitary probe now that the bladder is empty and take a look for the yolk sac or fetal pole. If the fetal pole has cardiac activity visualized then we can say it is a LIVE intrauterine pregnancy.