Happy Monday everyone! I mean, Tuesday!! Ugh! Well, if you were wondering where I’ve been, or even if you didn’t notice, I’ve had a busy couple weeks. From the many shifts that was full of interesting ultrasound cases (which you know I’ll share with you soon!) to graduating another stellar group of emergency residents, credentialing them in EM Ultrasound after 3 great years of training and a competency test, and hopefully soon to hear about the amazing pick-ups and lives saved in their future careers with the use of their great clinical judgement and bedside ultrasound. Im sure you love those busy weeks as much as we do, so i thought I would post something that would be a bit of positivity and highlight a group that I believe in: ACEP Ultrasound Section.
I’ll start with what I’ve said before: “2013 is the YEAR OF ULTRASOUND – and for good reason – there are only a few tools that give us such immediate information that can save a life. The ACEP US Section is the go-to site for everything you want to know about starting an US program, credentialing in ultrasound, the policies and politics, and is the home of SonoGuide – an amazing educational resource for bedside ultrasound, and the EMSONO: Ultrasound Test. It is also where we add our entries for their newsletter that goes over tips and tricks, cases, and all things ultrasound in the news. We recently wrote an article for the ACEP Ultrasound Section Newsletter – which is available for all members of the ACEP US Section – and I highly recommend becoming a member – it’s totally worth it. To continue to entice you, i will include our latest entry below – with a few additions in the end. For a set of links to online education in bedside ultrasound, go here. And, for our last entry into the Newsletter on Social Media in EM Ultrasound and the amazing tools out there to learn it for free, go here.”
Now, let’s talk about the FAST scan. It was a TRUE pleasure to record a podcast recently with Dr. Scott Weingart (aka, my hero) on EMCrit (twitter: EMCrit), and writing this article with our ultrasound fellow, Dr. Viveta Lobo, describes some of what was spoken about.
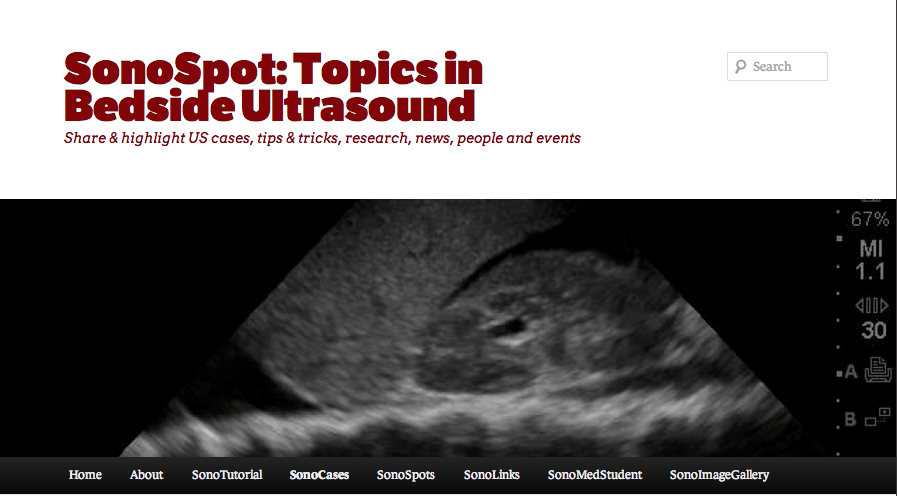
The focused assessment with sonography in trauma, or FAST exam, is undoubtedly the most widely used bedside ultrasound application in emergency medicine. With its incorporation into the ATLS trauma protocol, the FAST exam is performed immediately after the primary survey simultaneously with other resuscitative efforts. It is also a component of the RUSH protocol for patients with unexplained shock. Trauma patients often present with multiple injuries, and significant bleeding can occur without obvious changes in vitals signs. Medical patients can present intoxicated, altered, delirious, or demented all of which will limit the physical exam. The primary purpose of the FAST exam is to rapidly detect free fluid and hemorrhage in the peritoneal, pericardial and pleural spaces. There may be difficulties in obtaining adequate views, and we hope to discuss a few pearls to minimize them.
As with all ultrasound applications, familiarity with technique and patient anatomy, knowledge of common pitfalls, practice, and appreciating technical limitations are important errors to avoid. In general, the FAST exam is not “fast” – it can take up to 3-4 minutes to perform.1 The patient should be supine (or Trendelenberg) with low ambient light, with a low frequency probe used (the phased array probe provides the additional benefit of visualizing between the ribs and getting into the subxiphoid region more easily for the cardiac view). Even with the best technique, the FAST scan will only visualize 25 cc or more of thoracic free fluid and 500cc or more of intraperitoneal free fluid.2
The Right Upper Quadrant (RUQ)

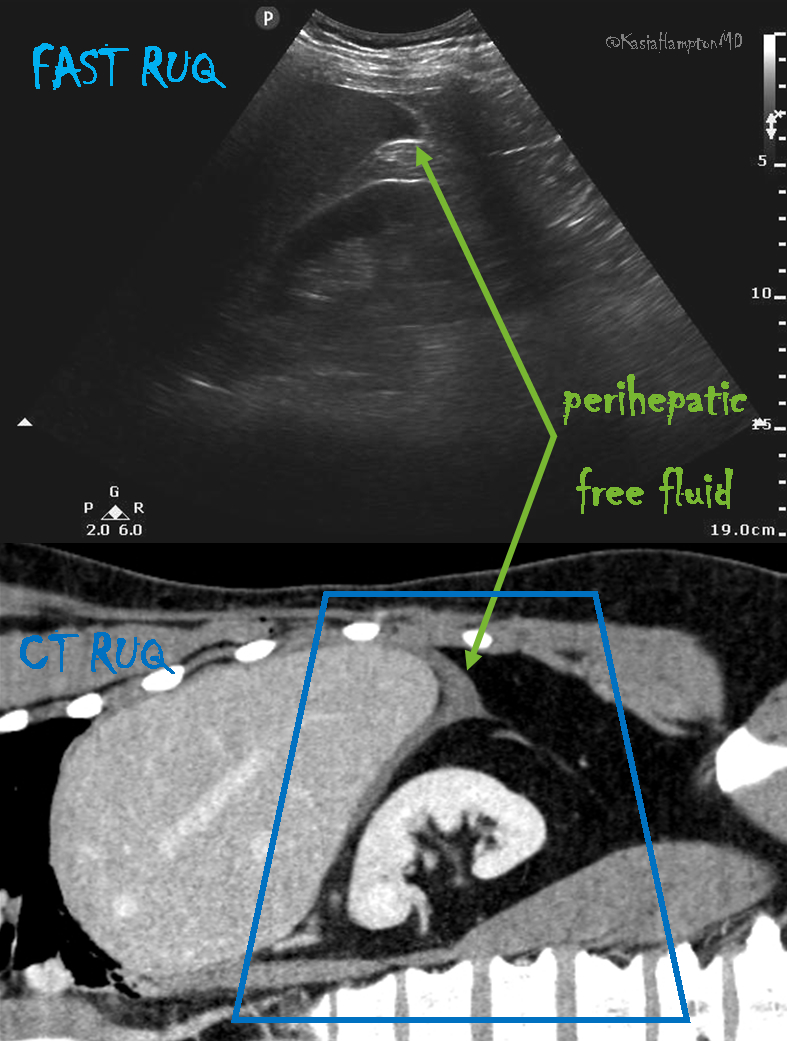
The RUQ is the most sensitive region for free fluid in comparison to the other FAST views.3 In my view, the RUQ should be divided into 3 zones.
1. Above/Below the diaphragm,
2. Morrison’s pouch (hepato-renal recess)
3. Paracolic gutter: Around the inferior hepatic edge/inferior pole of kidney
The key is to know your landmarks, and STOP, STAY and widely FAN through each zone well, adjusting your depth as necessary to keep the area of interest centered on your screen. Click Here for a Video. Start high to stay and fan (anterior to posterior) around the diaphragm. Then, SLIDE down into another rib space, stop, stay and fan around the entire kidney. An additional rib space may be necessary to evaluate the paracolic gutter.
Tips for RUQ Diaphragm View :
The liver may be easily seen, but the diaphragm can be more difficult, especially if it’s behind a rib shadow. Have the patient take in a deep breath. This lowers the diaphragm into your view and allows visualization of the thoracic cavity for hemothorax/pleural fluid as well as sub-diaphragmatic peritoneal fluid. Visualization of the spine shadow travelling in the lower part of the screen will normally stop at the diaphragm with a mirror image artifact illustrated in the thoracic cavity.

However, if the spine is able to been seen above the diaphragm– this is pathognomonic of pleural fluid, and also known as the “V-line.”4Click Here for a Video.

Tips for RUQ Morrison’s Pouch (Hepato-Renal Recess) View:
If rib shadows get in the way, using the same trick above of patient inspiration can help. There are also a few false positive “traps” here.
First, the double line sign, seen around the kidney capsule as hyperechoic double lines with hypoechoic material in between, can be mistaken for free fluid.5 However, free fluid will not be surrounded by hyperechoic lines and will not be in a contained structure.

Second, edge artifact from the liver/kidney interface occurs due to ultrasound physics and sound wave transmission between structures of different densities. It is seen as a dark thin line tracing off the edge of this interface extending to the bottom of the screen. Click Here for a Video. This differentiates it from free fluid, which will not extend past the liver.Click Here for a Video.

Tips for RUQ Paracolic Gutter View:
This is where free fluid can be seen first amongst all the different zones of the RUQ view.6The most important tip is to not forget to view this area. You will often have to slide your probe more inferior to obtain this view. Decrease the depth to look around the hepatic edge and inferior kidney pole, and evaluate the region with slow fanning. Click Here for a Video.

The Left Upper Quadrant (LUQ)
The LUQ is less sensitive for free fluid than the RUQ for varying reasons. First, the LUQ is opposite the side of the sonographer, which can make it technically difficult to obtain an adequate view. Also, the spleen is smaller than the liver and, thus, the acoustic window is lessened.

The stomach commonly obstructs the view as well. The LUQ should also be divided into 3 zones:
1. Above/Below the diaphragm,
2. Spleno-Renal recess,
3. Paracolic gutter: Around the inferior pole of kidney
Tips for the LUQ view
In addition to the various RUQ view tips and tricks as stated above, the LUQ diaphragm view also requires tips to avoid “stomach sabotage”. There are two ways around this: oblique the probe to have the indicator angled toward the gurney and/or slide your probe to the posterior-axillary line away from the plane of the stomach.

Look out for Part 2 of FAST Tips and Tricks, in the next newsletter where we talk about maximizing your cardiac views.
For additional material, images, and cases on the E-FAST, go here.
Another great review of FAST with excellent references here.
And, of course, saving the best for last – Cliff Reid and The Ultrasound Podcast discusses how to “earn your vaginal stripes” about the EFAST – go here.
Jacob Avila of 5MinSono did a great false positive blog on FAST here.
References
1. Boulanger BR, McLellan BA, Brenneman FD, et al. Emergent abdominal sonography as a screening test in a new diagnostic algorithm for blunt trauma.
J Trauma. Jun 1996;40(6):867- 874.
2. Branney SW, Wolfe RE, Moore EE, et al. Quantitative sensitivity of ultrasound in detecting free intraperitoneal fluid. J Trauma. Aug 1995;39(2):375-380.
3. Chambers JA, Pilbrow WJ. Ultrasound in abdominal trauma: an alternative to peritoneal lavage. ArchEmerg Med. Mar 1988;5(1):26-33.
4. Atkinson P, Milne J, Loubani O, et al. The V-line: a sonographic aid for the confirmation of pleural fluid. Crit Ultrasound J. 2012;4(1):19.
5. Sierzenski PR, Schofer JM, Bauman MJ, et al.
The double-line sign: A false positive finding on the focused assessment with sonography for trauma (FAST) examination. J Emerg Med. 2011;40(2):188-189.
6. Rozycki GS, Ochsner MG, Feliciano DV, et al. Early detection of hemoperitoneum by ultrasound examination of the right upper quadrant: a multicenter study.
J Trauma. Nov 1998;45 (5):878-883.

 1. Use your liver as an acoustic window.
1. Use your liver as an acoustic window.  Sound waves will travel through liver to the heart, allowing you to visualize the heart. Often one can even place the probe slightly to the right of the xiphoid process, to allow for better liver visualization, and then adjust your depth to be able to look past the liver to the heart. Without the liver in view, gas scatter will affect your image acquisition.
Sound waves will travel through liver to the heart, allowing you to visualize the heart. Often one can even place the probe slightly to the right of the xiphoid process, to allow for better liver visualization, and then adjust your depth to be able to look past the liver to the heart. Without the liver in view, gas scatter will affect your image acquisition.
 1. Start high and start medial – Place your phased array probe just next to the sternum, starting just under the clavicle. If you don’t see the heart there, slide down a rib space, and fan through that space to find the heart. Continue sliding down rib spaces, until you find it.
1. Start high and start medial – Place your phased array probe just next to the sternum, starting just under the clavicle. If you don’t see the heart there, slide down a rib space, and fan through that space to find the heart. Continue sliding down rib spaces, until you find it.

 Lastly, it can be very difficult in both subxiphoid and parasternal long views to differentiate epicardial fat pad from pericardial effusion. One tip: epicardial fat is seen anteriorly and has echogenicity within it, while pericardial effusion is seen posteriorly or inferiorly and is anechoic, but can travel anteriorly if large enough to become a circumferential pericardial fluid collection. Despite this tip, clinical correlation is needed.
Lastly, it can be very difficult in both subxiphoid and parasternal long views to differentiate epicardial fat pad from pericardial effusion. One tip: epicardial fat is seen anteriorly and has echogenicity within it, while pericardial effusion is seen posteriorly or inferiorly and is anechoic, but can travel anteriorly if large enough to become a circumferential pericardial fluid collection. Despite this tip, clinical correlation is needed.