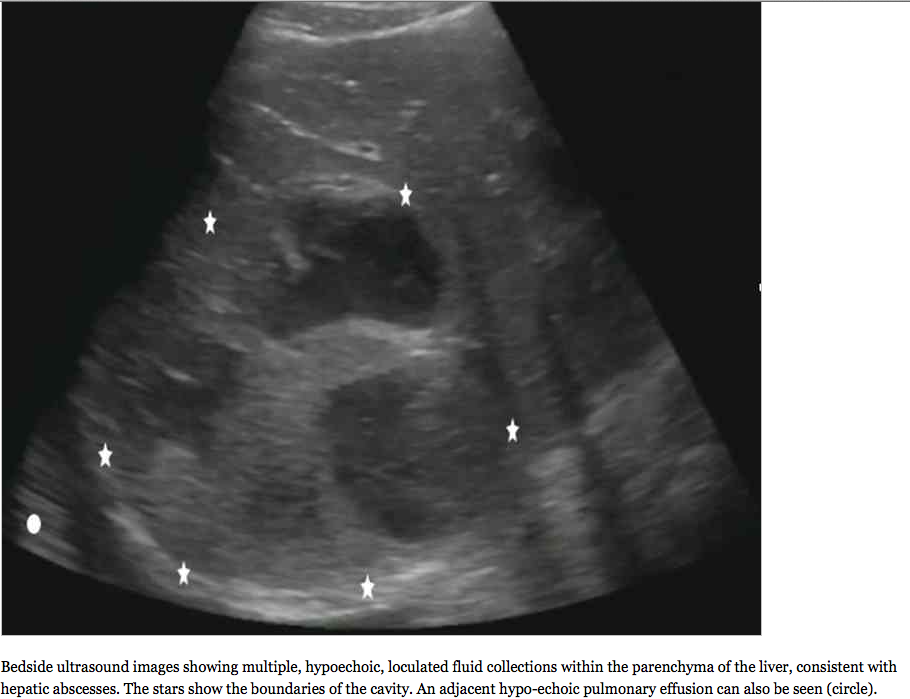
I keep thinking about this study published in the Jan 2013 issue of Academic Emerg Med by Dr. Nikita Joshi et al…. for a few reasons… so I thought i would highlight it on SonoSpot and spark some discussion to get your thoughts too. (Get full article here). First off, it’s about a condition that I see in the emergency department on every shift, so it’s incredibly relevant. And, it involves imaging, specifically ultrasound, and how it can benefit the patients with this problem from cost savings to quicker diagnoses and treatment. Finally, the results actually surprised me. Not because ultrasound seemed to be just as good as radiographs, but that they weren’t better. But, I should say that it was a meta-analysis and quite difficult to compare and the study subjects in the meta-analysis all had radiograph proven fractures, and I wonder what would have happened if the xrays were negative but the bedside ultrasound was positive, proven by a gold standard, like CT scan???…. Who am I kidding?! That would involve too much cost, radiation, and time in the emergency department….. Oh wait, I get it….I guess I understand the importance of this study now. There have been quite a few studies on the topic in the last couple years – go here, here, here, here, and here – which makes it really exciting.
The authors start by stating that radiographs do miss fractures:
“The typical work-up of the injured patient generally involves a medical provider obtaining a history and physical examination, often followed by radiologic imaging. However, many times the radiologic imaging may be negative or inconclusive, which calls to question whether the imaging contributed to the management or outcome of the patient. Studies have shown that often the imaging obtained is unnecessary and results in radiation exposure to patients and increased ED wait times.[2]….There’s a low rate of positive radiography when assessing for fractures as evidenced by a retrospective review by Bentohami et al.,[3] in which only 50% of upper extremity x-rays showed fractures, and another study by Heyworth,[4] which showed 15% of patients with ankle injuries had documented fractures on x-ray. In the study by Stiell et al.,[2] patients with ankle injuries had midfoot fracture rates of 4.3%, and 9.3% had malleolar fractures. Therefore, 50% to 95% of extremity x-rays can be avoided without missing fractures.”
Ok, so we know this. Xrays arent great, so why get them? If you think the fracture would need reduction due to a displacement, then ok. But, wouldnt that be possible by physical exam as a deformed extremity so that you’d know to Xray that one? If the extremity is not deformed, but tender and swollen, why not just splint? Isnt that what you would do anyway if the xray was negative due to a high clinical concern for “occult fracture”?
The authors then follow this up with one of my favorite paragraphs on the topic:
“Bedside US has the potential benefits of reducing radiation exposure, costs, and pain, while potentially improving ED patient throughput and satisfaction. This reflects on the original purpose of developing CDRs for extremity fractures. Use of bedside US can help triage patients during a busy ED shift by quickly assessing for the presence of fracture as an adjunct to the normal history and physical examination. It can also aid nurses and physicians who may require more resources for reduction of a fracture.[11] EPs have become more adept at fracture diagnosis through independent review of US and radiographic imaging, and many researchers have examined the ability of EPs to obtain US imaging and diagnose fracture.[12, 13] Additionally, bedside US has excellent diagnostic test characteristics when performed by EPs compared to radiologists in the diagnostic evaluation for soft tissue infections,[14] cholecystitis,[15] pneumothorax,[16] or ruling out ectopic pregnancy.[17]“
Love it. See the abstract below and read the entire article to see their limitations and methodology here.
Objectives
Understanding history, physical examination, and ultrasonography (US) to diagnose extremity fractures compared with radiography has potential benefits of decreasing radiation exposure, costs, and pain and improving emergency department (ED) resource management and triage time.
Methods
The authors performed two electronic searches using PubMed and EMBASE databases for studies published between 1965 to 2012 using a strategy based on the inclusion of any patient presenting with extremity injuries suspicious for fracture who had history and physical examination and a separate search for US performed by an emergency physician (EP) with subsequent radiography. The primary outcome was operating characteristics of ED history, physical examination, and US in diagnosing radiologically proven extremity fractures. The methodologic quality of the studies was assessed using the quality assessment of studies of diagnostic accuracy tool (QUADAS-2).
Results
Nine studies met the inclusion criteria for history and physical examination, while eight studies met the inclusion criteria for US. There was significant heterogeneity in the studies that prevented data pooling. Data were organized into subgroups based on anatomic fracture locations, but heterogeneity within the subgroups also prevented data pooling. The prevalence of fracture varied among the studies from 22% to 70%. Upper extremity physical examination tests have positive likelihood ratios (LRs) ranging from 1.2 to infinity and negative LRs ranging from 0 to 0.8. US sensitivities varied between 85% and 100%, specificities varied between 73% and 100%, positive LRs varied between 3.2 and 56.1, and negative LRs varied between 0 and 0.2.
Conclusions
Compared with radiography, EP US is an accurate diagnostic test to rule in or rule out extremity fractures. The diagnostic accuracy for history and physical examination are inconclusive. Future research is needed to understand the accuracy of ED US when combined with history and physical examination for upper and lower extremity fractures.
Nice job Nikita!
UltrasoundPodcast recently did a podcast on Distal radius fractures.
A great video of distal radius fractures can be seen here:
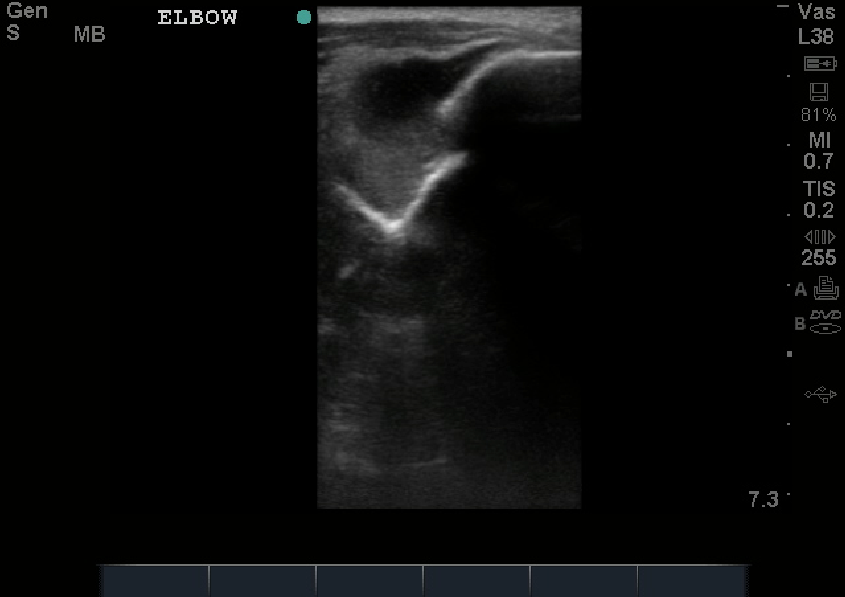
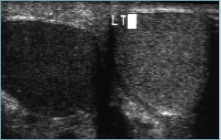
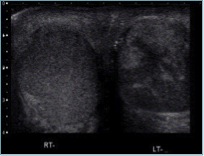
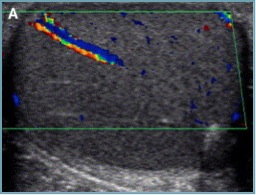
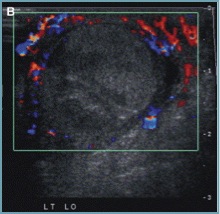
In case you’re curious about how easy it is to visualize a fracture by ultrasound, see image below. That bright white line is bone, and that break is …a break.

 and
and