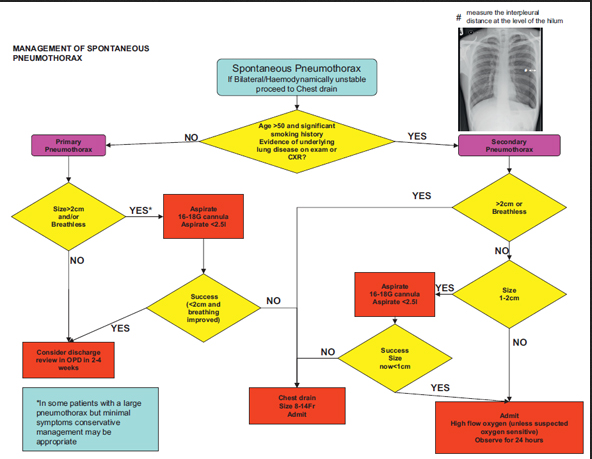
If there ever was a post worth reading about pneumothorax, this excellent review by EM Lyceum was too good not to pass along to everyone. Now I don’t know about you, but I always get asked the questions about chest Xray versus Ultrasound, what to do when only the ultrasound shows the pneumothorax (because you know it’s better than Chest Xray! as discussed in a prior post), when to order that CT chest, and how should you treat it: nothing? pigtail? small chest tube? large chest tube? EM Lyceum does a great job in reviewing this using literature to back it up. There have been more studies that haven’t been mentioned with regard to ultrasound and pneumothorax diagnosis, and the sensitivity and specificity of chest xray is stated pretty high as prior studies tend to do (with more accurate and recent ones stated by EM Lyceum to be lower (in the real world that we work in). And, there was a great meta-analysis in Chest Journal speaking of which imaging modality was better, chest Xray or ultrasound. Go to the EM Lyceum site and read-on to grasp the answers to all the questions! Thank you EM Lyceum – this was awesome!
The American Institute of Ultrasound in Medicine (AIUM) 2013 conference in New York City was the best AIUM I have ever been to, and it continues to open up my mind (having my ideas run wild!) to so many things that ultrasound will do for medicine, while reminding me of the up-to-date studies that clarify many ultrasound-related topics in medicine. It is true that Ultrasound should be considered first with many conditions, and as an emergency physician, point-of-care bedside ultrasound is definitely an example of that. It absolutely should also be implemented into medical school education to have a head-start at becoming an excellent physician. AIUM has an emergency and critical care section too and I have taken full advantage of the information there, as should you. (Jason Nomura has gathered all AIUM13 tweets for your reading pleasure for all AIUM13 topics)
YOU = Year of Ultrasound!
This post is a one part of a 4-Part Series where I discuss all the lectures, panel discussions, and events that i attended there, and what every emergency doctor should get out of it, and the literature that backs it up or discusses the controversy – all through my and other’s twitter feed with the addition of some links to relevant material.
The first day was one of my favorites! It was the Ultrasound in Medical Education panel discussion from the experts, coordinated by Dr David Bahner, who has recently published study after study after study after study with regard to how he incorporated ultrasound into medical education and how to standardize ultrasound education. You can even listen to and view the whole course if you have an AIUM membership, by going here. Dr. Richard Hoppman, the Dean of University of South Carolina, who has also published study after study after study after study on this topic, also gave his pearls and wisdom from the Dean’s perspective. (Hear/View his interview with UltrasoundPodcast by going here.) Other experts also gave their expertise in this hot topic, as they have also published and highlighted study after study after study after study as shown below in the tweet and panels’ pearls from the course (as well @SonoMedED tweets who provided more highlights for the course): Ultrasound in Medical Education (I posted on the comparison of Ultrasound to physical exam previously – but there is so much I need to add to it now!)
a. Provide clinicians with resources to guide medical student training in clinical ultrasound to better provide care for their patients
b. Provide educators with the resources and tools to coordinate clinical ultrasound in medical curricula
c. Provide researchers with evidence based resources to create and validate new knowledge through innovative and rigorous academic pursuits
d. Provide administrators with data and contact personnel at respective medical institutions who are applying novel ultrasound education across the medical spectra
e. Provide medical students with a one-stop portal to navigate current United States medical student ultrasound education and opportunities to get in school
1. David Bahner – This would involve changing curricula, training faculty, acquiring equipment, support staffing, quality assurance, OSCE or SDOT, establish “best-practices.” In 2004, the medical organizations differentiated & defined ultrasound into four categories: Comprehensive, Focused, Procedural, Physical exam aid
2. D. Lichtenstein – “They call me Dr. Lung, but I do more.” There are exciting ways to show medical students the importance of ultrasound….New territories of ultrasound: mesenteric ischemia (“a bowel that doesn’t move is a dead bowel”), pneumoperitoneum, increased ocular use. Took 15 publications in order to publish the BLUE protocol that reviews 10 signs of lung US. Respiratory failure: BLUE http://crashingpatient.com/wp-content/uploads/2011/07/Lichtenstein-Slides.pdf … ; Circulatory failure: FALLS (if no B lines then good systolic fxn; if B lines then bad systolic function); Cardiac Arrest: SESAME protocol (lung sliding (if pneumothorax- immed interv), echo, then IVC and AAA at your discretion: http://www.slideshare.net/nswhems/the-arrested-patient … Lung Ultrasound in Critically Ill for Limiting Radiographs (LUCIFLR) project – to decrease CT and chest Xrays (but not to eradicate Xrays “or LUCIFLR will = LUCIFER”). Lung ultrasound can limit the need for chest X-rays in the ICU and the ED.
3. Creagh Boulger – speaking on literature review of ultrasound curriculum for medical students. MT “@SonoMedED: Medical students effectively use ultrasound in just 5 min in some situations.” [Even beating clinicians in diagnosis! See: this study.] . Study after study has shown that medical students benefit from ultrasound in medical education. How to fit it into the schedule? what they did – online didactics (like Fox’s iTunes series), then 16 weeks of hands-on, concluded with a checklist based assessment. Why teach it? Increases Anatomy Learning, increases diagnostic ability in radiology, assists in spatial relationships, and they see “live anatomy” with better ability to learn physiology in real-time.
5. John Pellerito – how to incorporate US into med school: buy in from Dean, faculty training, facility space, US equipment, MULTI-specialty involvement (emergency medicine, radiology, critical care, obstetrics, medicine, surgery). US in med school: online didactics, most time must be spent with hands-on: knobology, anatomy, physiology, pathology (- partner with pathology /radiology dept to show how ultrasound correlates with histology/specimens and CT/MRI [they will learn to read those better too by learning ultrasound!]). Society of US in Med Ed (SUSME) website to see sample curriculum. The Challenges of incorporating US into Medical Education: maintenance of longitudinal curriculum, keep faculty enthusiastic, budget for new equipment, space needs. MT“@SonoMedED: Challenges with med stud ultrasound educ 4yr curriculum, keep faculty interested. pic.twitter.com/UnRSCGs0vk”. Who to Train them? First will be faculty, then the seniors can teach the juniors. Essentials im developing an US curriculum: didactics and hands-on training, integration into anatomy, physiology, physical exam and diagnosis skills, clinical clerkships, and requires student assessment and image archiving and review. Faculty/Facility needs: classroom, bedside, anatomy lab, stretchers, gel, towels, monitors, models (students or patients), faculty from multiple specialties
6. Amponsah/Jackson – from Wayne State : how they incorporate US in med stud curriculum: didactics, 2nd yr competency test, multi-specialty involvement. Where US helps med stud in anatomy learning: spatial relations, pathology, live anatomy pic.twitter.com/MCI972lryO . Need high faculty:student ratio. LCME requirements are key to getting ultrasound into medical school:
LCME requirements are a great way to advocate for ultrasound education as part of active learning for medical students …..The following LCME requirements can be satisfied with ultrasound: ED-5-A: A medical education program must include instructional opportunities for active learning and independent study to foster the skills necessary for life-long learning; ED-12: The curriculum of a medical education program should include laboratory or other practical opportunities for the direct application for the scientific method, accurate observation of biomedical phenomena, and critical analysis of data; ED-28:A medical education program must include ongoing assessment of medical student’s problem solving, clinical reasoning, decision making, and communication skills.
7. J. Christian Fox – From UC Irvine. pic.twitter.com/znUAea1wew . Bridging the gap between pre-clinical and clinical students with simulations: How to do it: transitioning from pre-clinical to clinical medical students: podcast, then hands-on with healthy volunteer, then task trainer, then recognize pathology on simulator, then standardized patient with pathology, then clinical rotation utilization by way of an OSCE pic.twitter.com/ix4Rl2X4WS “Sono-genic” models great to use- models with great US anatomy. Issues in real patients: obesity, COPD, pain- all limit scan ability but great for later training. Great models: Sono-Studs… Or, not so good: Sono-Mess MT“@SonoMedED: Terms for good sonographic models…Sonogenic…Sonolicious.” (Ah, I digress…). Solve issue of assessing pathology: simulation! Various simulators are on the market: http://Sonosim.com , http://bluephantom.com ,http://Vimedix.com , http://www.medaphor.com/ , http://www.medsim.com/ultrasim.html . MT “@SonoMedED: Dr. Fox signs up pts for modeling with various pathologies. Model pts with pathology compensated $80 for 4 hour session. Often challenging to schedule patients though.” Great way to get models who have pathology! Studies show increasing ultrasound performed in ED when increased medical student ultrasound learning, also that liver span size better when use ultrasound. Medical students are better with ultrasound in diagnosing cardiac disease when compared to cardiologists’ physical exam.
8. Michael Blaivas– The role of specialty organizations- AIUM, SUSME, WINFOCUS, and specialty specific: ACEP, SAEM, ACS, ACOG, ACCP, SCCM, Card, Rads. http://SUSME.org primary purpose is integrating US into med educ. http://WINFOCUS.org primary purpose to help proliferation of Ultrasound education, is worldwide, has detailed US educ curriculum, policy making depending on region/country. Summary- issues and specialty organization – how they help pic.twitter.com/ZsO9BKWa6B
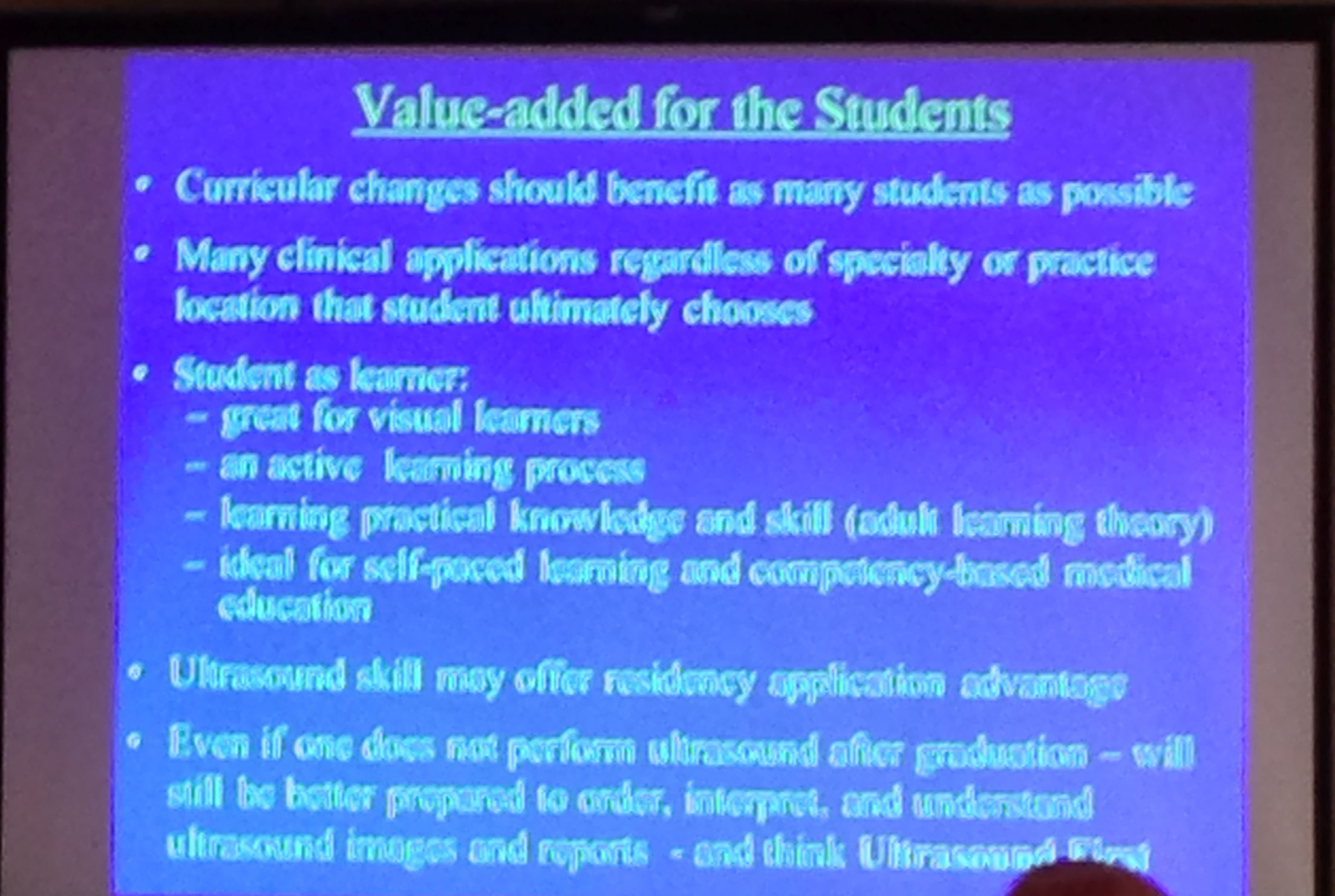
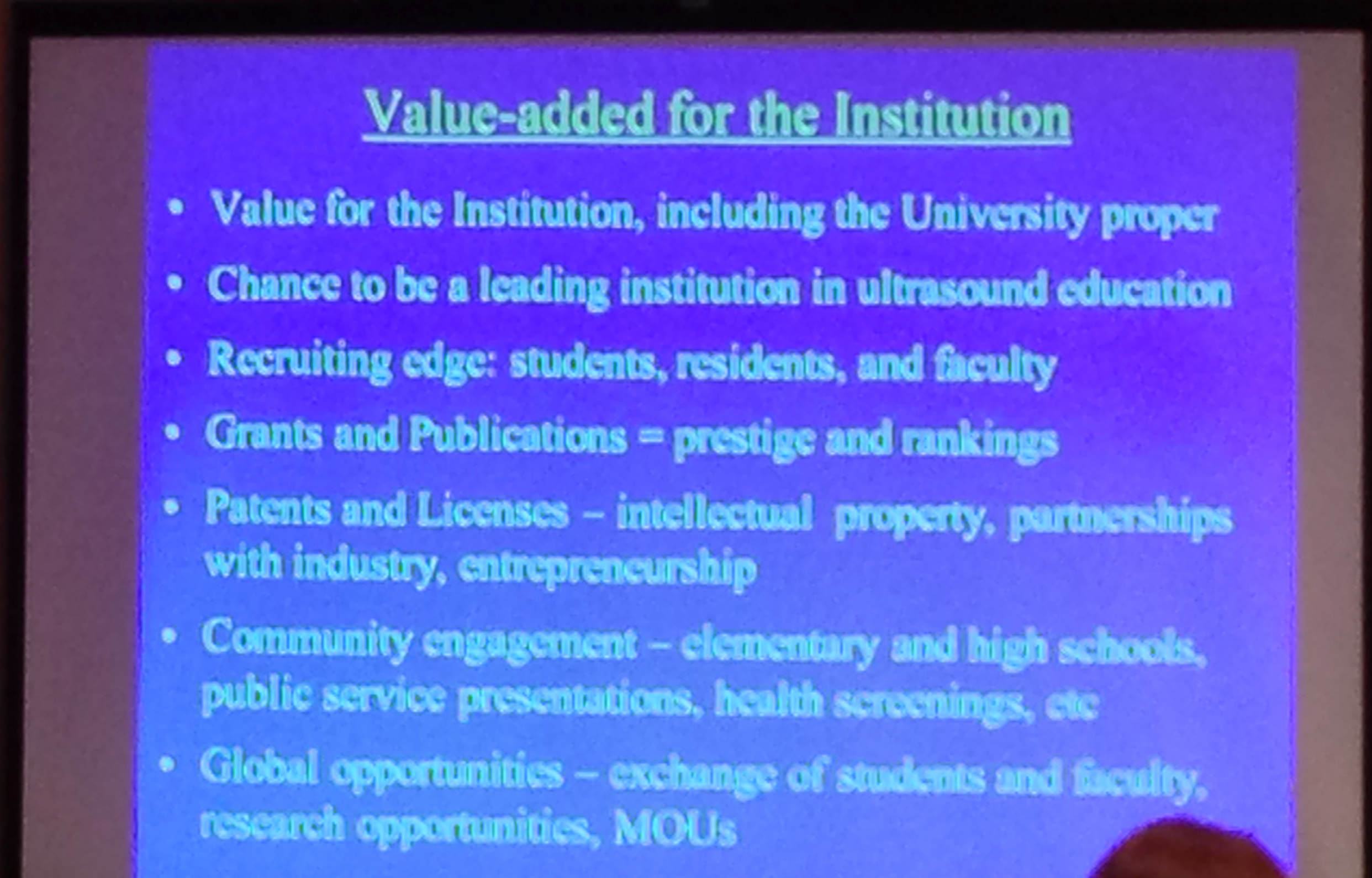
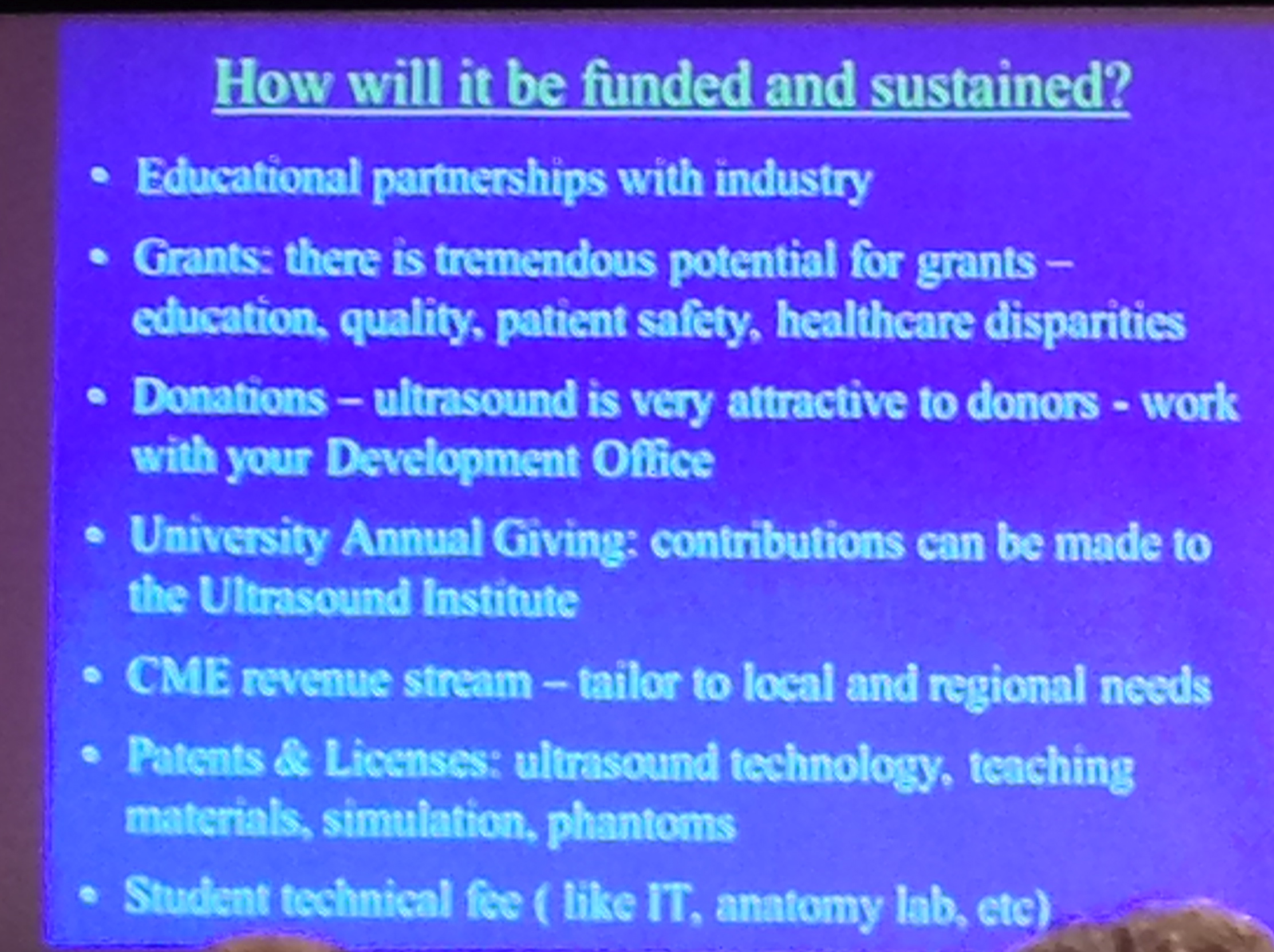
9. Dean Richard Hoppman – from University of South Carolina: pic.twitter.com/hAx4Iqv9rR . US in medical education- A Dean’s Perspective, how to get them on your side: how to get US in medical education- get medical students on your side, show US enhances medical education, satisfies LCME requirements, fits all types curriculum. When ultrasound becomes part of Step 2 exams is when you know we’ve arrived… [Wow! Can u imagine?!]….Ultrasound competency could be an advantage to residency application. Even if they don’t use US in residency, can order/ interpret/understand ultrasound and other radiology studies better, they’ll think Ultrasound First! How ultrasound adds value to institution pic.twitter.com/dzJt0VAaNE . Hopefully one day ultrasound training will be a requirement for medical school graduation. How to fund ultrasound for your institution pic.twitter.com/uItTHJj2Jb . MT“@SonoMedED: Universities increasing focus on entrepreneurship. patent ultrasound ideas or devices. Help fund program” Great idea by Hoppmann -> MT “@SonoMedED: Advocate option for donors to contribute to medical school ultrasound programs.”The new stethoscope? MT“@SonoMedED: Grants supply equipment for med studs, even handheld units. pic.twitter.com/5t9wbOtsef” medical students love it, medical students become alumni, alumni become donors. Great way to advocate for it pic.twitter.com/TnxBLjhsJn. Dean’s summary message to all: Get it. Learn it. Do it. Teach it. For your patients & healthcare pic.twitter.com/LfUQv2SbJK . Yes!!-> “@SonoMedED: Great insight from Dean Hoppmann. pic.twitter.com/VcW1BUmbRl”
10. Teresa Liu – from GW (the one who is putting it all together for med studs at AIUM/SAEM/ACEP). White paper on ultrasound in medical student education is in progress. ACGME now incorporates ultrasound into EMed and RRC doing same for rheumatology. Medical students can get involved in specialty organizations/journals focused in ultrasound: JUM, Acad Med, SUSME/SAEM/AIUM/ACEP. Lower cost-Increased use! -> MT“@SonoMedED: Liu- need for making US tech more affordable to better penetrate into all specialties.”
11. Alex Levitov– curriculum and competency assessments: challenges & opportunities. Driving force for ultrasound are many clinical cases where it’s relevant & when time matters: its a busy day or patient critical.When people ask why – tell them this: pic.twitter.com/CUth7L3Vxj . US allows immediate diagnosis, immeidate data in patient care, & allow reassessment after intervention (CVC placement, chest tube, foley…). Competency in US- image acquistion in years 1/2 ; Simulators, clinical cases & they decide what to do next for years 3/4. US in meded-cardiac physiology usually rated low by medical students, but rated high after ultrasound used to enhance education. Best way to incorporate US in medical education- staged approach -& use clinical cases early, ask about interventions in clinical years
12. Vicki Noble– from Mass General – discusses Ultrasound Competency –NEJM article -Point of Care Ultrasonography shows how many use it . “Numbers” for image acquisition competency- should it exist? Arguments for & against exist. Outcome need to be different? “Consensus is great, paralysis is bad”-concept of plateau-do more of same if literature show numbers don’t matter may mean we should change. US competency numbers may be different for different ultrasound applications; numbers may not matter for some applications- testing image interpretation requires clinical integration & “next step” questions. Online ACEP US test: http://www.emsono.com/acep/exam.html
13. James Palma– from Georgetown – web based & organizational considerations in ultrasound in med ed – organ based approach – online didactics; hands on. web based US curriculum pic.twitter.com/l9fuWycluk
14. Last but not least – MEDICAL STUDENT PANEL !! Medical students panel discussing how #ultrasound helps them -going into different specialties pic.twitter.com/4B8IjKjtTQ . Ultrasound helps spatial relations in anatomy, great for MSK in real time (ie. rotator cuff movement), heart great to match with physiology (“it’s hard to understand heart physiology by reading a book, and so much better when you see the valves opening and closing and how the heart pumps”) . Great to see kidney ultrasound because anatomy dissection takes all abdominal organs out & can’t appreciate spatial relations. “@SonoMedED: Med Student Panel-Ultrasound physiology best demonstrated for IVC collapsibility and ejection fraction.” When asking medical student their preference: separate course versus full integration in different classes with regard to ultrasound into medical education: all wanted the latter – unanimously! . Story by a medical student: Psychiatric ward patient w/ abdominal pain got hand-held ultrasound by medical student showing cholecystitis- comprehensive ultrasound confirmed; OR that day. MT“@SonoMedED: Med Stud Panel-key to making integration of ultrasound successful: make it clinically relevant in 1st/2nd year.” “Ultrasound makes me feel that I can contribute to the team.”
15. Prior advances in Ultrasound in Medical Education has been highlighted by others: I have posted about how ACEP, AAMC, and AIUM last year has started speaking about ultrasound in medical education; UltrasoundPodcast have a great podcast about it and how to incorporate it here and here; WesternSono posted about this from the Canadian perspective with an amazing and fun talk pitching ultrasound training in medical education here; the world is advancing this goal as well!
Some of the great slides that grabbed my attention from the AIUM13 course: (apologies for the blurry iPhone images)
The Medical Student Panel:
The Course’s Faculty: aka – the All-Stars!
And, to conclude with great insight and words of wisdom for why ultrasound should be in medical education:
And what he has done to spread the gospel of ‘sound! – go here to read more and hear a speech done by the Dean of UC Irvine Medical School on why its so important to incorporate ultrasound into medical education for our patients.
Im off! New York City, here I come! AIUM 2013 is right in the heart of Times Square: where the lighted ball drops on every new year, where Madonna was taken as a young girl after telling the cab driver “Take me to where everything happens”, and where hundreds of healthcare providers from different specialties come together this year who all believe in ultrasound, and discuss when/where ultrasound should be used FIRST – as described in the UltrasoundFirst Forum. This is a big deal this year. Why? Well, you see, and as some of you may already know, 2013 is the Year of Ultrasound (YOU)! There were quite a few events I posted about earlier speaking of this great event/year, which was so greatly put into practice by my good friend who taught me everything I know about ultrasound, Dr. Chris Fox, at UltraFest this year – a free medical student ultrasound course (yup, that’s right, FREE). 2013 – The year that we should spread the gospel of ‘sound to areas where it is so needed, in global health practice, in medical school education, to community physicians to help guide their screening, resuscitation, procedures, and diagnosis of their patients – to EVERYONE who will listen!
So, in preparation for this event, as discussed with one of my role models, Dr. Richard Hoppmann, for how he incorporated ultrasound into medical education, a curriculum that is described in the Society of US in Med ED (SUSME) website, we thought how fun it would be to get as many people as we know to wear the 2013:YOU T-shirts and post it for everyone to appreciate! He sent us the shirts, the Stanford US team put them on, and had great fun with the photo-shoot! Look out for more folks to post photos like these throughout the week! – if they so dare….
Then, it got a little fun….. 🙂
The great Dr. Vicki Noble and her team at Harvard/Mass General also had a fun Photo-shoot! Love the shirt on the machine!….
Drs. Abdi, Stacy, Mailhot, and Perera once again describe a case where ultrasound made the difference in clinical management of a patient. Their case is published in WestJEM with a great tutorial video (see below) accompanying it.
Emergency physicians perform bedside ultrasound in 1st trimester abdominal pain and vaginal bleeding to “rule in” an intrauterine pregnancy, but the better way to describe how we think about it is “ruling out” any signs of an ectopic pregnancy. By doing it in the emergency department, it has been shown to decrease length of stay of these patients, and increase their satisfaction. With a full bladder, a transabdominal pelvic ultrasound is performed with a regional assessment of the pelvic organs to visualize for confirmation of an intrauterine pregnancy (yolk sac or fetal pole within a gestational sac in the uterus). You may need to empty the bladder and perform a transvaginal ultrasound if the above does not provide the information you need (I bring the ultrasound machine with me to the bedside when I first meet them so that I can do the history, physical, and ultrasound right off the bat). If there is an identifiable pregnancy then an evaluation for a fetal heart and its rate is assessed in order to characterize it as a “live” intrauterine pregnancy. But, if there is no contents within the gestational sac (a potential pseudosac), or if there is no gestational sac, then the concern for ectopic pregnancy still exists. Of course, in a recent post, we discuss that even those cases may turn out to have a normal pregnancy despite an elevated beta hcg level, calling into question whether the “discriminatory zone” should be used to guide our management.
Let’s go back to their case: The brilliance of this case, however, isn’t that they found an ectopic or illustrate what I describe above, instead it illustrates that there are other diagnoses that may be apparent on ultrasound that is causing the pelvic pain and vaginal spotting. And, if you don’t look, or if you are unfamiliar with what you are seeing on the screen, you may miss it – or mistakingly call it an intrauterine pregnancy.
The case: 32 yrs old G1P0 known pregnant at 7weeks by last menstrual period with lower pelvic cramping and vaginal spotting. A bedside ultrasound is performed and the video below describes what they saw…. read more on the case here.
Since “being pregnant” is a diagnosis that can be made, we shouldn’t stop there after we have identified an intrauterine pregnancy. We shouldn’t simply state “you’re pregnant” and discharge them home without further consideration of the etiology of their pelvic pain. Something else may be causing it. (to read about other cases using pelvic ultrasound, go here.) Other findings/diagnoses to consider in 1st trimester pelvic pain or vaginal spotting:
1. Ovarian cyst or torsion (see this case report in J of EM that discussed exactly why you should continue to evaluate with bedside US).
This SonoGift is amazing! I could have sworn that I sent this earlier (and I think i did on Twitter and Facebook), but for whatever reason, it is in my blog’s draft folder, and I was shocked! – How dare I keep this away from everyone who follows SonoSpot?!!!! So, I apologize… from the bottom of my subxiphoid window (…ha! yes i know, I have many of them). If you’re getting this for the second time, then take it as a friendly reminder of how awesome the UltrasoundPodcast guys are to provide this amazing gift to everyone to learn the up-to-date info on bedside ultrasound applications… for free. Now, if you are getting this for the first time, you are going to LOVE it….. Why? Well, first off, it’s free (did I say that already?). And, if that wasnt enough, it’s the pdf version of the AWESOME iPAD download-able iBook (also found here chapter by chapter purchasing on inkling that can also been read on iPHONE) of Introduction to Bedside Ultrasound from the UltrasoundPodcast crew, with chapters written by so many of my friends. If you purchase the iPAD version (for pretty cheap, if you ask me) (including the iPAD mini and retina display), you can view all the clips and videos placed by the authors/experts in bedside ultrasound – which truly makes it the best “book” on bedside ultrasound that I know. It’s worth it.
You know what else Im excited about? SonoGames Part Deux at SAEM – this time, our crew is going to make it after the first round!!! You all better watch out! A sneak peak at SonoGames last year by the serious yet humorous, heavy yet light, good yet talented UltrasoundPodcast and their hilarious interviews:
Oh, and did I mention Castlefest2013????!! Im so excited to join them at CastleFest2013 – ultrasound, castles, wine, and festivities?—what more could a Sonogirl ask for?! You can even be there virtually! Yes, they did think of everything.
Drs. Teresa Wu and Brady Pregerson (in the current issue of EPMonthly) once again discuss an interesting case that is more than meets the eye, and thankfully they continue their humorous sarcasm and start the case by speaking of an average day in our emergency departments these days: “This is the third time this week that you have had to close your ED. All of the beds in the hospital are full, and your ED is bulging at the seams with sick patients that aren’t going anywhere anytime soon. You are holding 10 admissions at the present moment, and the hallways are lined with patients calling “doctor” every time you walk by. As much as you hate doing so, you concede to the request to close to ambulance traffic and then walk briskly over to the chart rack to see what you can do to help improve the current situation. Your eager intern is right on your heels and says he has a new patient to present to you. “This should be a really simple case,” he spurts out. You raise your eyebrows and bite your tongue.”……
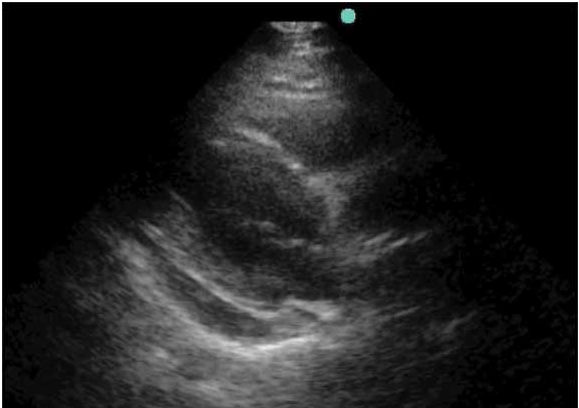
They (meaning, the intern) describe a case of a 40 year old female who has had what seems like an upper respiratory infection for 4 weeks, that’s just not going away, and now with sharp chest pain worse when coughing. While going to evaluate the patient, they give one of the best pearls that all residents should know: ““Teaching point number one is conservation of energy. One of the best ways to be efficient is to ensure that you minimize the amount of time wasted. If you might need the ultrasound machine, take it with you so you don’t have to walk back out of the room to go get it.” They then proceed to perform the beginnings of the RADIUS study, which highlights Echo, thoracic and IVC ultrasound for the short of breath/dyspneic patient. The patient complains of pain when lying back, which causes the spide-y sense to go up and be confirmed when seeing the below picture on the echo:
To read more on the case and their great clinical pearls click here to get to EPMonthly’s online site.
To read a prior post emphasizing the need to perform an ultrasound for any presumed or confirmed pericarditis by going through a another case… and some studies, click here.
Not that we didnt already know this, but at least we have more data to say it is so – in a recent study in Annals of Emergency medicine – a meta analysis reviewed 9 trials – both kids and adults.
This concept has been getting a lot of press, and many of my ultrasound enthusiast friends have passed this around. It’s good to know the concept – and use it when you are in a conversation with someone who thinks the blind technique it still the way to go.
“Pediatric trials yielded conflicting data, the authors reported February 18 online in Annals of Emergency Medicine, but there appeared to be significantly fewer attempts and shorter procedure times when ultrasound guidance was used in the emergency department, as well as significantly decreased risk of first-attempt failure, reduced attempts, and shorter procedure time when ultrasound guidance was used in the operating room…..”Ultrasonographically guided peripheral intravenous cannulation may perform better in the pediatric population because failure rates with the traditional method are much higher in children than adults,” the researchers note. “Ultrasonography may not be as beneficial in adults, in whom target vessels are easier to locate.” – Now, these trials were from operating room patients, where the setting is a bit more controlled, the patients may be a bit different in their difficult IV access spectrum – but the authors still suggest that if faced with a difficult IV – use ultrasound.
Below is the abstract:
Study objective
Peripheral intravenous cannulation is procedurally challenging and painful. We perform a systematic review to evaluate ultrasonographic guidance as an aid to peripheral intravenous cannulation.
Methods
We searched MEDLINE, Cochrane Central Register of Controlled Trials, EMBASE, Cumulative Index to Nursing and Allied Health Literature (CINAHL), Web of Science, ClinicalTrials.gov, and Google.ca. We included randomized trials evaluating ultrasonographically guided peripheral intravenous cannulation and reporting risk of peripheral intravenous cannulation failure, number of attempts, procedure time, or time from randomization to peripheral intravenous cannulation. We separately analyzed pediatric and adult data and emergency department (ED), ICU, and operating room data. Quality assessment used the Cochrane Risk of Bias Tool.
Results
We identified 4,664 citations, assessed 403 full texts for eligibility, and included 9 trials. Five had low risk, 1 high risk, and 3 unclear risk of bias. A pediatric ED trial found that ultrasonography decreased mean difference (MD) in the number of attempts (MD −2.00; 95% confidence interval [CI] −2.73 to −1.27) and procedure time (MD −8.10 minutes; 95% CI −12.48 to −3.72 minutes). In an operating room pediatric trial, ultrasonography decreased risk of first-attempt failure (risk ratio 0.23; 95% CI 0.08 to 0.69), number of attempts (MD −1.50; 95% CI −2.52 to −0.48), and procedure time (MD −5.95; 95% CI −10.21 to −1.69). Meta-analysis of adult ED trials suggests that ultrasonography decreases the number of attempts (MD −0.43; 95% CI −0.81 to −0.05). Ultrasonography decreased risk of failure (risk ratio 0.47; 95% CI 0.26 to 0.87) in an adult ICU trial.
Conclusion
Ultrasonography may decrease peripheral intravenous cannulation attempts and procedure time in children in ED and operating room settings. Few outcomes reached statistical significance. Larger well-controlled trials are needed.
For more info and a how-to for ultrasound guided procedures, including ultrasound-guided peripheral IV and central IV acces – go here.
I saw an interesting blog post, sent to me by my ultrasound uncle, Dr. Chris Fox, that was on the: “Why Is American Healthcare so Expensive?” site entitled “How to Make Ultrasound gel: which is also sterile and edible and environmentally friendly” by Dr.Janice Boughton. Not only did the title catch my eye, but the content drew me even closer. If you are in need of gel – whether that’s because you are doing global health, disaster relief, or healthcare at any resource-limited area – there are ways to make it. Ive heard of a couple alternatives – and here is a way to make your own – that is also sterile, edible, and environmentally friendly. 🙂
As the blog post states: “Ultrasound requires an aqueous interface between the transducer and the skin or else all you see is black. Ultrasound gel is a clear goo, looks like hair gel or aloe vera, and is made by several companies out of various combinations of propylene glycol, glycerine, perfume, dyes, phenoxyethanol or carbapol R 940 polymer along with lots of water.” – not easy to find, and ot so cheap either. So, she set out and tried six different recipes – yup, that’s right – SIX! …and made the below gel (see pic) from guar gum (found in the flour section of stores), salt and water:
“Guar gum is available in the flour section of many grocery stores and costs about $10 for a 220 gram bag. It is purported to be good for diarrhea, constipation, diabetes and lowering cholesterol.” – how cool is that?!
1. Mix 2 teaspoons of guar gum with 1-2 teaspoons of salt. (The amount of salt isn’t vitally important since it is just added to keep the guar gum from clumping. Using slightly less than a teaspoon of salt per 2 cups makes a gel with which is isotonic, which would be ideal for use near eyes or other mucus membranes or on open wounds).
2. Boil two cups of water.
3. Slowly sprinkle the guar gum/salt mixture into the boiling water while stirring vigorously with a fork or whisk.
4. Boil for about 1-2 minutes until thick and well mixed.
5. Cool before using. Save lives.
To read more about her plight – click here. Thanks Janice!
Wireless communication in medicine, smartphones for ECG monitoring and healthcare screening, portable ultrasound use in the clinic at the bedside instead of a patient sent to an ultrasound suite on a separate date – all resulting in quicker, more efficient, and cheaper medicine. Dr. Eric Topol, a cardiologist practicing in Scripps hospital in San Diego (my hometown – oh yeah!) – tells Rock Center with Brian Williams on NBC about it all and MORE! – the future of medicine is amazing and so incredibly exciting! – wireless medicine is just the beginning – what patients can do at home to screen for various diseases wirelessly is only one part of the future – he speaks of how this all saves money too – very interesting interview! Too good not to share! http://www.nbcnews.com/video/rock-center/50582822#50582822
Dr. Topol also discusses the top 5 devices that every patient and doctor should get to know, as they will take over the world of healthcare as we get more and more digitized (of course, one of the devices is a hand-held ultrasound machine!)
In a recent article in the European Journal of Emergency medicine, the authors showed that emergency physicians are just as good as radiologists in detecting small bowel obstruction by bedside US. Now, it’s not hard to do, nor is it hard to see it. First off, use your abdominal low frequency probe, and evaluate the abdomen in different quadrants. Normally, the bowel appears as a single circular hypoechoic layer (muscle layer) surrounding hyperechoic bowel contents of gas and food particles. The normal thickness of this layer during the contraction stage of peristalsis is 2-3 mm. The hypoechoic normal wall becomes thinner during peristalsis when the bowel is relaxed.
In small bowel obstruction- looking for dilated fluid filled loops of bowel with hyperechoic (bright) spots within it that may have back and forth peristalsis and a thicker intestinal wall (decreased persitalsis is a late finding) – color doppler gives info about blood flow in the walls of the intestine – and you may even see a transition point. Timothy Jang and team studied ultrasound compared to Xray for SBO and found that ultrasound is better, like WAYYYY better (higher sensitivity and specificity) – hmmm, interesting – Some things to consider: fluid-filled loops (good for US), but air-filled loops may not be so good. Ileus and SBO may appear similarly, so consider thinking of causes of ileus as well (gallstone ileus, etc), and a thickened wall may just be colitis, but that along with dilated loops and back and forth persitalsis with a transition point seen – more likely SBO.
This is what it would look like (and there are more clips to view – thanks to SonoCloud)
The abstract of the study follows:
“Objective: Our objective was to study the accuracy of emergency medicine [(EM) bedside ultrasonography (BUS)] and radiology residents performed ultrasonography (RUS) in patients with suspected mechanical small bowel obstruction (SBO).
Methods: After a 6-h training program, from January to June 2009, four EM residents used BUS to prospectively evaluate the patients presenting to the emergency department with suspected SBO. Then, patients underwent RUS. Outcome was determined by surgical findings if they were operated upon or self-reported the condition upon telephone follow-up at 1-month. BUS and RUS results were compared with χ2 testing.
Results: Of the 174 enrolled patients, 90 patients were BUS-positive. Of these, surgical findings agreed with the BUS findings in 84 patients. In 78 cases, BUS was negative, and 76 of these patients had benign clinical courses. Six patients were excluded from the study. The sensitivity, specificity, positive predictive value, negative predictive value, and likelihood ratio for BUS were 97.7, 92.7, 93.3, 97.4, and 13.4%, respectively. Sensitivity, specificity, positive predictive value, and negative predictive value for RUS were 88.4, 100, 100, and 89.1%, respectively. The diagnostic accuracy of BUS and RUS were not statistically different from each other (κ=0.81). The presence of dilated small bowel loops (>25 mm in jejunum or >15 mm in ileum) was the most sensitive (94%) and specific (94%) sonographic finding for SBO.
Conclusion: Abdominal sonography for the diagnosis of SBO is a new application of BUS in the emergency department. EM residents can diagnose SBO using BUS with a high-degree of accuracy, comparable with that of radiology residents.”
To read the UltrasoundPodcast guys speak on the subject, click here>