In the most recent issue of WestJEM, a very interesting ultrasound case by Drs. Wendler, Schoenberger, Mailhot and Perera was published illustrating that if you dont look, you won’t get the diagnosis! How bedside ultrasound solved the case! Below is only the beginning of the case:
“A 57-year-old Hispanic male presented with a 1-day history of altered mental status. He had a past medical history significant for alcohol abuse, hepatitis C and Child-Pugh Class B cirrhosis. He had undergone TIPS placement an unknown number of years before presentation to the ED. Additionally, he had been previously hospitalized for hepatic encephalopathy due to noncompliance with his medical regimen.
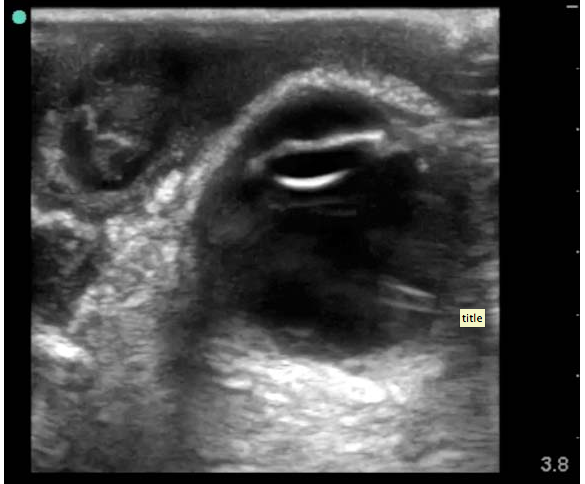
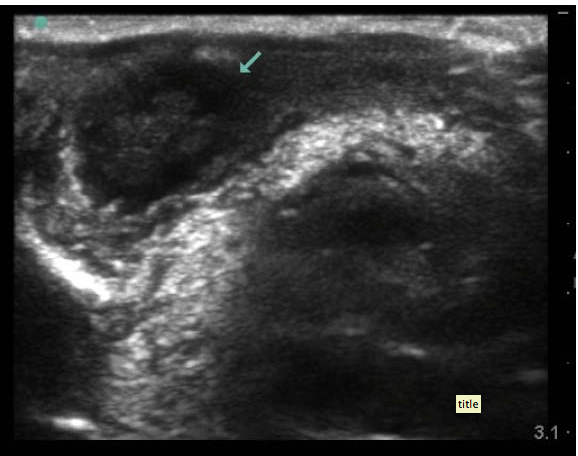
On physical examination, the patient appeared comfortable and calm. He was alert, but oriented to name only. Vitals signs were temperature 98.1°F pulse 78 beats/ min, respiratory rate 16 breaths/min and blood pressure 130/89 mmHg. The patient was noted to have scleral icterus, and his abdominal exam revealed moderate ascites without tenderness, rebound, or guarding. Unexpectedly, on cardiac auscultation, the patient was noted to have a 2/6 systolic and a 2/6 diastolic murmur with ectopy. A 12-lead electrocardiogram (ECG) was obtained in addition to standard laboratory studies to elucidate the cause of the patient’s altered mental status.
The serum white blood cell count was 6,500/mm3 without neutrophilic predominance, hemoglobin of 10 g/dL, BUN of 10 mg/dL and a creatinine of 0.6 mg/dL. The patient was noted to have an elevated ammonia level at138 umol/L. The 12-lead ECG showed normal sinus rhythm with multiple premature atrial contractions. To further assess cardiac function, a bedside EUS was performed…..” (see below)
Oh, but there’s more! The case isnt over, nor the discussion – read more!
In the Feb 2013 issue of Chest, Oveland et al studied porcine models, introducing air at incremental levels to identify if thoracic ultrasound is as accurate as CT scanning for the detection pneumothorax progression in the intubated patient. They found that “the accuracy of thoracic ultrasonography for identifying the lung point (and, thus, the PTX extent) was comparable to that of CT imaging. These clinically relevant results suggest that ultrasonography may be safe and accurate in monitoring PTX progression during positive pressure ventilation.”
“Background: Although thoracic ultrasonography accurately determines the size and extent of occult pneumothoraces (PTXs) in spontaneously breathing patients, there is uncertainty about patients receiving positive pressure ventilation. We compared the lung point (ie, the area where the collapsed lung still adheres to the inside of the chest wall) using the two modalities ultrasonography and CT scanning to determine whether ultrasonography can be used reliably to assess PTX progression in a positive-pressure-ventilated porcine model.
Methods: Air was introduced in incremental steps into five hemithoraces in three intubated porcine models. The lung point was identified on ultrasound imaging and referenced against the lateral limit of the intrapleural air space identified on the CT scans. The distance from the sternum to the lung point (S-LP) was measured on the CT scans and correlated to the insufflated air volume.
Results: The mean total difference between the 131 ultrasound and CT scan lung points was 6.8 mm (SD, 7.1 mm; range, 0.0-29.3 mm). A mixed-model regression analysis showed a linear relationship between the S-LP distances and the PTX volume (P < .001).
Conclusions: In an experimental porcine model, we found a linear relation between the PTX size and the lateral position of the lung point. The accuracy of thoracic ultrasonography for identifying the lung point (and, thus, the PTX extent) was comparable to that of CT imaging. These clinically relevant results suggest that ultrasonography may be safe and accurate in monitoring PTX progression during positive pressure ventilation.”
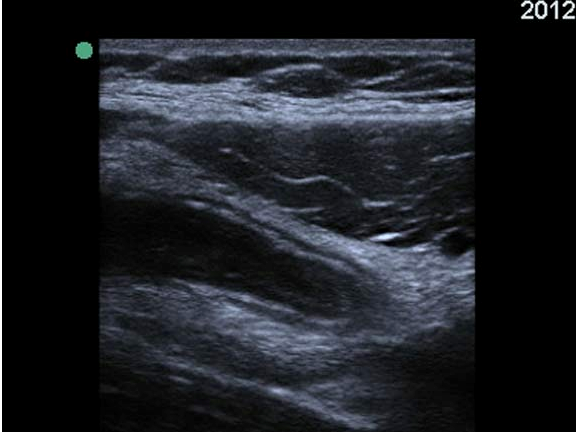
To see the lung point, you visualize the pleural line using the linear probe (indicator toward the patient’s head) starting from anterior chest wall (2nd intercostal space, mid-clavicular line) to inferior-lateral chest wall, and look out for the area where the lack of lung sliding or comet tail artifacts reverts back to normal lung sliding with comet tail artifacts. Blaivas, et al, studied this, showing that bedside ultrasound can detect size of pneumothorax through identification of the lung point location. Below is a video fo the lung point:
In the recent issue of WestJEM, a case report of another excellent application for bedside ultrasound is described by our very own Dr. Phil Perera (yup, he is more than just the RUSH exam). A video where he discusses the ultrasound application and case follows….
“A 35-year-old man presented to the emergency department (ED) for acute urinary retention and penile pain for 4 hours. The patient denied any significant medical history or history of trauma. Physical exam revealed testicles that were nontender, without masses. However, a tender mass was felt at the distal end of the penis, adjacent to the urethral meatus. Placement of a Foley catheter resulted in a return of 700 cc of clear yellow urine and immediate resolution of the patient’s suprapubic and penile pain.
During the ED course, the Foley catheter was removed with a subsequent trial of voiding. Initially, the patient was able to void 15 cc of urine until the normal stream was abruptly cut off. The patient then complained of extreme penile pain, near the urethral meatus. A small, circular and firm mass was again palpated in the distal penile shaft. Bedside emergency ultrasound (EUS), performed with a 10 MHz linear array probe placed along long axis of penis, revealed a hyperechoic, dense and round structure with characteristic acoustic shadowing at the distal end of the urethra, with obstruction of the urinary flow (Video). The object, a 9 mm stone, was removed with forceps. Following stone removal, the patient experienced immediate pain relief and was able to spontaneously void.
While urethral imaging has traditionally been performed with retrograde urethrography (RUG), more recently ultrasound has been used to minimize the pain associated with RUG and to provide clinicians more detailed information about urethral pathology.2 As demonstrated in this case, EUS allowed a prompt diagnosis of the patient’s condition with appropriate rapid treatment and removal of the urethral stone.”
In a recent study in Pediatric Emergency Care, the folks at newark Beth Israel in New Jersey studied whether performing a pelvic ultrasound decreases length of stay. Now, we all can appreciate this – you have a pregnant patient with first trimester vaginal bleeding or abdominal pain, you see an intrauterine pregnancy without any risks/signs of heterotopic (which is incredibly rare anyway) – you’re done! You dont even have to wait for the beta hCG! Of course that decreases length of stay! Now, this wasnt the first study of it’s kind. Another study by Blaivas et al. basically did the same thing… 13 years ago! And by Burgher…. 16 years ago. And by Shih…. 16 years ago! There was a great review of pelvic ultrasound done in 2009 that shows its accuracy and utility too.
Well, here is what they state: abstract below
“OBJECTIVES: Diagnostic ultrasounds by emergency medicine (EM) and pediatric emergency medicine (PEM) physicians have increased because of ultrasonography training during residency and fellowship. The availability of ultrasound in radiology departments is limited or difficult to obtain especially during nighttime hours. Studies have shown that EM physicians can accurately perform goal-directed ultrasound after appropriate training. The goal of this study was to compare the length of stay for patients receiving an ultrasound to confirm intrauterine pregnancies. The hypothesis of this study is that a bedside ultrasound by a trained EM/PEM physician can reduce length of stay in the emergency department (ED) by 1 hour.
METHODS: This was a case cohort retrospective review for patients aged 13 to 21 years who received pelvic ultrasounds in the ED during 2007. Each patient was placed into 1 of 2 groups. Group 1 received bedside ultrasounds done by institutionally credentialed EM/PEM attending physicians. Group 2 received radiology department ultrasound only. Each group had subanalysis done including chief complaint, time of presentation, time to completion of ultrasound, length of stay, diagnosis, and disposition. Daytime was defined as presentation between 7 AM and 9 PM when radiology ultrasound technologists were routinely available.
RESULTS: We studied 330 patients, with 244 patients (74%) in the bedside ultrasound group. The demographics of both groups showed no difference in age, presenting complaints, discharge diagnoses, and ultimate disposition. Group 1 had a significant reduction (P < 0.001) in time to complete the ultrasound compared with group 2 (mean, 82 minutes [range, 1-901 minutes] vs 149 minutes [range, 7-506 minutes]) and length of stay (142 [16-2268] vs 230 [16-844]). Of those presenting during the day (66%), group 1 showed a significant reduction in length of stay (P < 0.001) compared with group 2 (220 [21-951] vs 357 [156-844]). Of those who presented at night (34%), group 1 showed a significant reduction in length of stay (P < 0.002) compared with group 2 (270 [16-2268] vs 326 [127-691]).
CONCLUSIONS: The use of ED bedside ultrasound by trained EM/PEM physicians produced a significant reduction in length of stay in the ED, regardless of radiology ultrasound technologist availability.”
Some interesting cases for your review:
SonoCase: 30 yr old with pelvic pain, LMP 5 weeks ago, stable vitals, mild tenderness in suprapubic area, pelvic exam normal. Your Transabdominal pelvic view on ultrasound shows the below. What do you do next?
Well, we see a full bladder – which is a must if you actually care about your pelvic views – and we see a gestational sac with a double decidua sign – the earliest sign of an intrauterine pregnancy, BUT it is not enough to diagnosis a definitive intrauterine pregnancy – you need a yolk sac within your gestational sac to say that! So, get your endocavitary ultrasound probe and take a look (after emptying the bladder), you may just see the yolk sac!
SonoCase: 24 yr old with pelvic pain, LMP 6 weeks ago, stable vitals, mild tenderness in suprapubic area, pelvic exam normal. Your Transabdominal pelvic view on ultrasound shows below. What is the diagnosis? What do you do next?
Well, there is an empty bladder (unfortunately), so the visualization is not its best, but while we slowly fan through the pelvis there is a fluid filled circular cystic-like structure with mild acoustic enhancement (brightness deep to it) which allows you to also see a gestational sac within the uterus. There is an ovarian cyst. Is that what’s causing the pelvic pain? Are you sure it’s not an ectopic? Not yet – get your endocavitary probe now that the bladder is empty and take a look for the yolk sac or fetal pole. If the fetal pole has cardiac activity visualized then we can say it is a LIVE intrauterine pregnancy.
In the most recent issue of EP Monthly, Drs. Teresa Wu and Brady Pregerson, give another enlightening and humorous story of the average every-day emergency patient after first describing how they explained to their EM intern the role of emergency physicians (which I couldnt agree more with!): “As an EM physician, you are a healer, an educator, a detective, a diagnostician, and a master strategist all rolled into one.”
The case:
“41-year-old male who presents to the ED with concerns that his left eye is progressively getting more swollen. He’s had some increasing eye pain and purulent drainage over the past six days. At first he thought that he was just having really bad seasonal allergies, but today, he started feeling a “pulling sensation” on the medial aspect of his left eye. He denies any headache, diplopia, sinus pain, rhinorrhea, nausea, vomiting, or recent trauma. He does note a subjective fever at home, and his temperature is 38.2°C in the ED. His vital signs otherwise demonstrate tachycardia to 123 bpm, but a normal blood pressure, oxygen saturation, and respiratory rate. Your intern has asked the nurse to obtain a visual acuity on the patient and he is systematically going through his ocular exam when you walk by the room to check on him. He comes out of the room to give you an update on what he’s discovered so far. The patient has tenderness to palpation over his left medial orbit and possible entrapment on ocular exam. He has no additional pain with extraocular movement and no diplopia, but has so much periorbital edema that it wasn’t possible to get a consistent Tonopen measurement. There doesn’t appear to be any fluorescein uptake on the slit lamp exam, and other than conjunctival injection and the lid swelling, the patient has a normal ocular exam.
It is now about 4:30 pm and you know that in 30 minutes, all consultants turn into pumpkins and their pagers magically stop working. As you are about to ask your intern what he wants to do next, the medical student pulls up the ultrasound machine that the intern asked her to wheel over and hands it to him. He takes the linear array transducer and performs an ocular ultrasound at the bedside. He saves the following images: what do you see?”
To find out…..and read up on what it was, what happened, and the pearls of the exam, go here.
Merry Christmas everyone! For your reading pleasure this week, Id thought we would discuss a case whose topic is near and dear to my heart. In the most recent issue of EPMonthly, there is a great case and interesting “internal” discussion made quite humorously public by Drs. Pregerson and T. Wu of a young healthy male with right lower quadrant abdominal pain after eating at a “Roach Coach”…. which just so happen to have the best breakfast burritos, but I digress… The case discussion involves how the history and physical may help, how labs may (or may not) help and how an ultrasound can be of use to make you and your surgical colleagues feel better in taking the patient to the OR. There was a recent post on SonoSpot about ultrasound in appendicitis sharing data from a study about the CT findings when US “equivocal” cases arise. When the ultrasound is positive – how great is that?! Quite a few studies recently on the topic and some of the more recent ones can be found here.
The case is followed by an extensive (and great) discussion of the technique, pearls and pitfalls of ultrasound in evaluating the appendix – because we all know there are quite a few. As far as the sensitivity ad specificity go, they state it best:
“Sensitivity & Specificity: Both the sensitivity & specificity of ultrasound for appendicitis are less than that of CT. In pediatrics the values are about 88% and 94% respectively, and in adults about 83% and 93%. (These numbers may vary depending on the experience of the ultrasonographer.) There are studies from Europe and Israel where they have used the “ultrasound first” approach for many, many years that show even better test characteristics. These values are actually not that bad when compared to CT scan whose sensitivity and specificity are around 94% and 95% respectively. Remember, however, that the performance characteristics for ultrasound can be significantly worse in overweight patients or those with overlying bowel gas. In addition, if the appendix is retrocecal or is lying in a difficult anatomical plane, the study will be more challenging. Unfortunately, you may still have to do a CT scan if your ultrasound is non-diagnostic and your clinical suspicion is moderate to high, but the strategy of ultrasound first would likely decrease CTs by about 50%.”
And in kids…”You should be aware of the most recent recommendation of the American College of Radiology from the “Choosing Wisely” campaign, which states, “Don’t do computed tomography (CT) for the evaluation of suspected appendicitis in children until after ultrasound has been considered as an option.” Although CT is accurate in the evaluation of suspected appendicitis in the pediatric population, ultrasound is nearly as good in experienced hands. Since ultrasound will reduce radiation exposure, ultrasound is the preferred initial consideration for imaging examination in children. If the results of the ultrasound exam are equivocal, it may be followed by CT. This approach is cost-effective, reduces potential radiation risks and has excellent accuracy, with reported sensitivity and specificity of 94 percent.”
To diagnose appendicitis: look for a noncompressible a-peristaltic structure that attaches to the cecum that is larger than 7mm in diameter.
A great tutorial of ultrasound for the appendix can be found here by the UltrasoundPodcast guys:
I’d like to introduce everyone to our amazing Ultrasound Fellow, Dr. Viveta Lobo (otherwise known as “VLo” to our team – of course!). She came to us by way of Drexel, tolerates out antics, appreciates our quirks, and laughs at our jokes. We love her! Enjoy this post about a healthy guy who looked very sick, short of breath, and only bedside ultrasound, using the RADIUS protocol, could help diagnose it so quickly and get the patient what he needs and fast….
I’m about 4 months into my Ultrasound (US) Fellowship at Stanford, and while I am thrilled to have greatly improved my US skills, and image acquisition during a scanning shift, it is in no comparison to the thrill, and satisfaction I felt, after using my bedside US skills to navigate through the following case.
A 55-year-old healthy male, with no past medical history, presents with progressively worse shortness of breath over the past 2 weeks. Within 30 seconds of being in the room, he is getting more short of breath, dusky, diaphoretic, and requiring to now sit up and lean forward while speaking to me in 1 word sentences. He is on a 100% non re-breather, sating about 93%. The rest of his vitals – BP 124/84 RR 41 HR 124 Temp 97.8
Even as a new attending, I was pretty certain, that if I did not figure this out in the next few minutes, this once very healthy patient is going to decompensate, and likely end up with grave morbidity. However, given that he had no known history, I had nothing to go by, except…. I grabbed my US probe, and within 3 minutes, I gained a wealth of information. I first took a look at his chest by using the phased array low frequency probe on each side of his chest in 8 total areas (4 on each side). This is what I see throughout:
…. >2 large B lines bilaterally, rays from the pleural line on the top to the end of the screen.
When I switched to a RUQ and LUQ views, my suspicions were confirmed :
RUQ:
LUQ:
…Now, the US images are on cardiac presets so the resolution is a touch different than what we are used to, but the findings are obvious which heightened my concern for the patient even more: large pleural effusions noted bilaterally. Seen as a black (anechoic) area above the diaphragm. Black is fluid on ultrasound, and you can even see the lung trying to breathe on each of the images above.
Next, I quickly assessed his IVC, and saw a plump dilated IVC, consisted with fluid overload state, which prompted me to stop my nurse from hanging any IV fluids. I then performed a bedside echo:
Subxiphoid view: (placing the phased array low frequency probe in the subxiphoid area and pressing down while flattening the probe, using the liver as an acoustic window to see the heart):
Apical 4-chamber view: (placing the probe just underneath the nipple line, at the point of maximal impulse and angling toward the body center):
…. I was able to rule out a pericardial effusion and cardiac tamponade as well as any significant RV strain to suggest a hemodynamically unstable pulmonary embolism, but I appreciated significant left ventricle dysfunction, and hypokinesis.
I then took a look using the linear probe on the anterior chest wall at the 2nd intercostal space and saw:
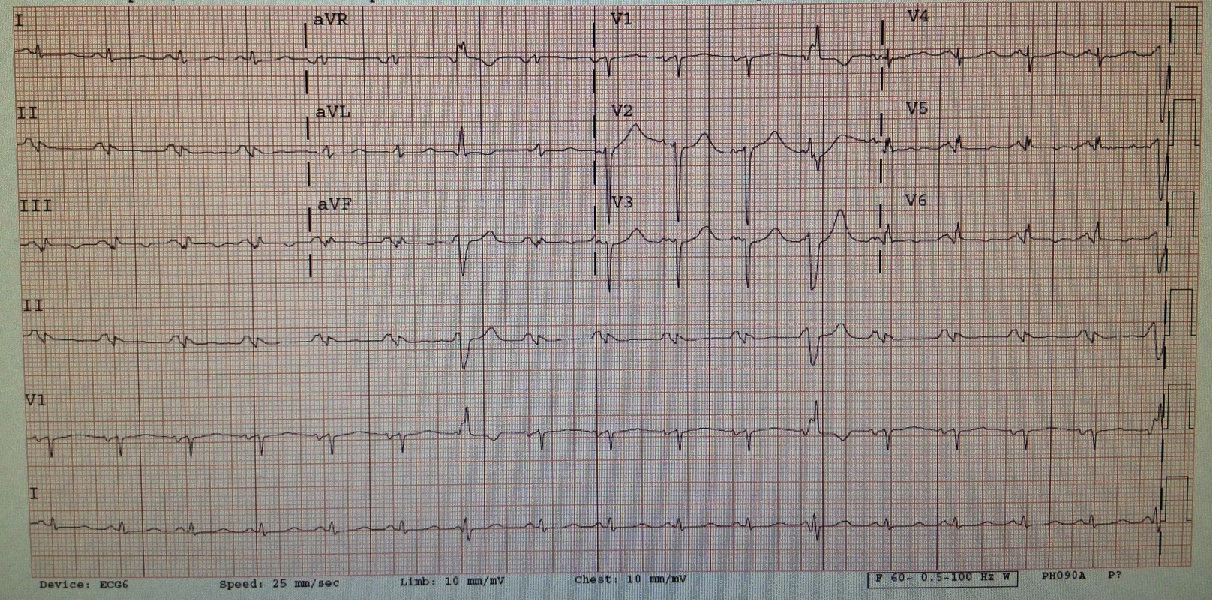
So, there is great lung sliding but we see it almost too well! The reason is because fluid is the lover of ultrasound and will allow you to see tissue deep to it better due to enhancing of echoes. There is fluid between the parietal and pleural layers, more and more from superior to inferior chest – on both sides. That’s quite a bit of pleural effusion if it goes all the way up to the upper lung zones! While I was putting the pieces together and realizing the diagnosis, my nurse informs me that his istat troponin comes back elevated. His initial EKG:
…..showed sinus tachycardia with ischemic changes inferior and laterally, with t waves inversions. We also see multiple PVCs. No old one EKG for comparison. Ah, the evolution of an MI on EKG – love it!
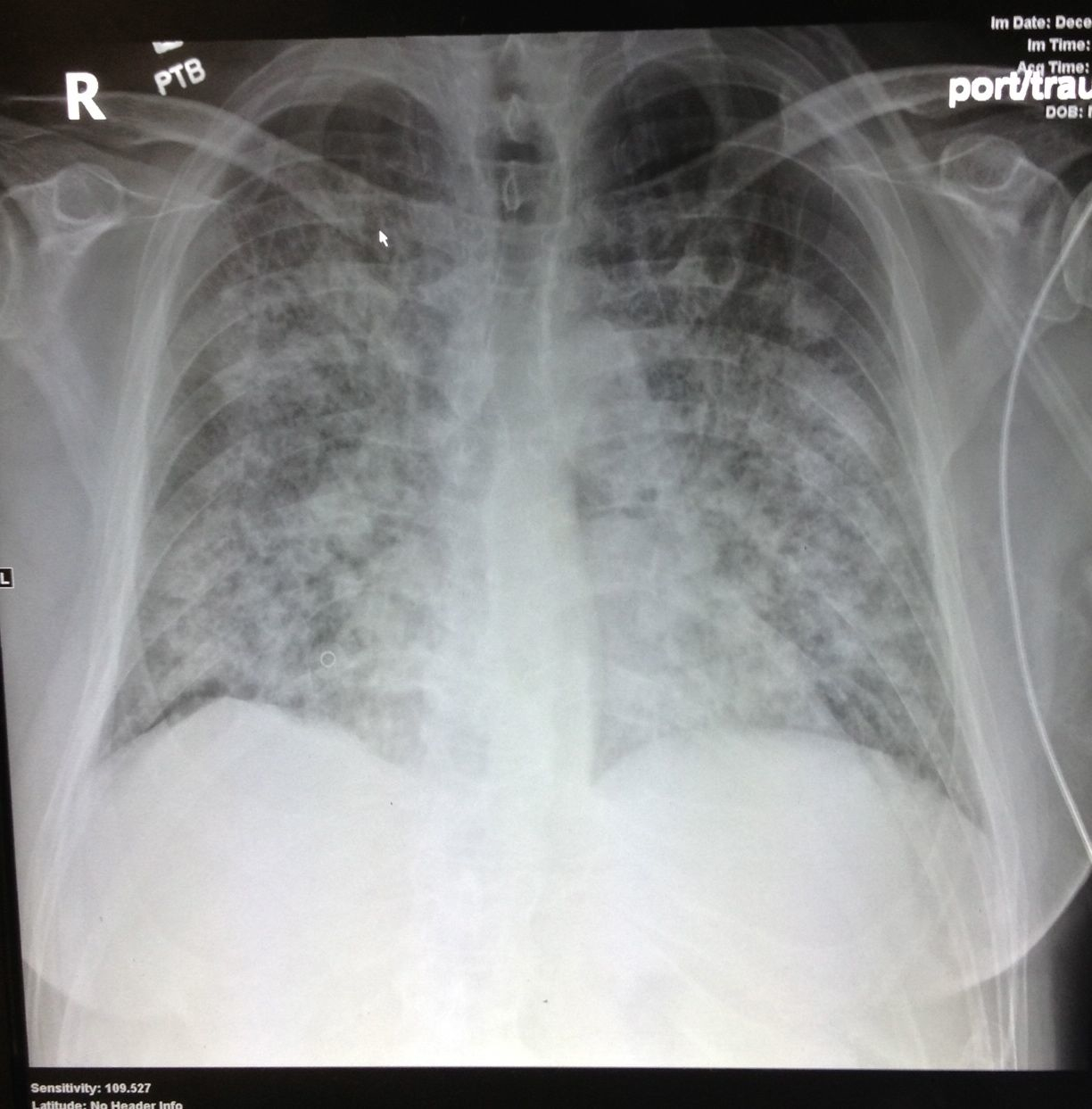
So to recap, I have an otherwise healthy gentlemen, with progressive sob, no chest pain, but with positive family history of ACS, with confirmed LV dysfunction on US and bilateral pleural effusions and a positive troponin, and some possible ischemic changes on EKG. Sounds like a post ischemic cardiac event presenting with ventricular infarct! From door to diagnosis in 5 minutes! I placed him on BIPAP, gave him a big shot of Lasix IV, aspirin PO, and called my cardiologist! The patient started to improve after the medication, avoiding intubation. The Chest Xray was then done:
….showing bilateral diffuse opacities which could be typical for ARDS.
After a brief cardiology evaluation, my patient was admitted to the CCU and shortly after went to the Cath lab, and was found to have a complete LAD occlusion.
While I initially had a very broad differential including PE, new onset CHF, cardiac tamponade, myocarditis, pneumonia; my bedside ultrasound was quickly able to prioritize my differential, and consult the right service, with a specific question of – should this patient go to the cath lab? Without bedside US, this patient could have easily been a Medical ICU evaluation for respiratory distress, with an extensive work up, including CT Chest, intubation, and more time than the patient needed for a diagnosis to have bee made while we sorted through the differential.
This case is one of many that completely validates bedside ultrasound for me, and my decision to pursue this awesome fellowship!
As a follow up: Patient went on to get an LVAD, and is on the heart transplant list.
In the most recent issue of EPMonthly, our good friend, Dr. Teresa Wu, and Brady Pregerson right up a case they had of a patient with abdominal pain. In their wisest and most sarcastic way, they present this case with a great teaching point (ok, there are many teaching points as you will find on the last page of the case – but one in particular that deserves special mention). Read on and see if you can get what that point may be…
“56-year-old otherwise healthy female who presented to the ED with a chief complaint of “severe abdominal pain” after she finished lifting boxes of heavy books at her job the day before. She states her pain is worse with movement and is better when she lies still. She has never had pain like this before, and today, it is 10 out of 10 in severity. The pain is described as sharp and tearing, but it does not radiate to her chest or back. She has no other associated symptoms, and she has tried Ibuprofen without any relief.
Her vital signs are all completely within normal limits and her physical exam is only remarkable for tenderness to palpation over her left rectus muscles, and a seemingly pulsatile aorta palpable through her thin abdominal wall. She has no rebound or guarding on abdominal exam, and she has no other abnormal findings. Given her symptoms and her palpable aorta, your senior resident decides it would be prudent to do a quick scan of her aorta to make sure nothing catastrophic is imminent.” The following image was obtained:”
The Aorta seems ok. Hmmmm…..Still wonder what happened to the case and what it was? Read the issue in depth and you’ll then get to know and love Teresa Wu as much as I do.
Hint – look at the entire screen when evaluating any organ by bedside ultrasound…..
In the most recent installment of the Sound Judgement Series by AIUM, Drs. Rochelle F. Andreotti and Sara M. Harvey from the Department of Radiology at Vanderbilt discuss the use, accuracy and effectiveness of ultrasound for acute pelvic pain. It seems that pelvic pain has, again, become an important issue as there are quite a few articles that have come out about it recently, likely because there are so many visits to clinics and emergency departments with this exact chief complaint. As the authors state “The diagnosis can be challenging because many symptoms and signs lack sensitivity and specificity. Urgent life-threatening conditions requiring surgical intervention (eg, ectopic pregnancy, appendicitis, a ruptured ovarian cyst, and ovarian torsion) and fertility-threatening conditions (eg, pelvic inflammatory disease [PID] and ovarian torsion) should take precedence over other disorders.” – Guess which imaging modality can evaluate all of them? Continue reading →
An article that just recently came to my attention made me start to think a little bit about how we teach how to do the FAST scan. In a prior post, I discuss the RUQ and LUQ details – to ensure to not miss any amount of free fluid that should be seen on the FAST scan, keeping in mind it’s limitations. Then, I read this article in the EMJ online First from April 2012 that discusses a case of an ‘unusually’ positive FAST scan, but when reading about the injury and the location, I am not surprised about the location of free fluid development. Hind-sight is 20/20, but it highlights a few key concepts that should always be addressed: look for free fluid in the REGION on the RUQ and LUQ, not only between the liver/spleen and kidneys AND serial FAST scans for any patient where the mechanism suggests a risk for intra-abdominal injury (particularly if you are not going to CT the patient) – I do this frequently in the patients who come in drunk as all get-out where I cannot rely on my physical exam or the pediatric population where radiation would be best avoided if possible.